Robotics in Orthopaedic Surgery – Brief Summary
By Dr. Pothireddy Surendranath Reddy, Orthopaedic Surgeon
1. Introduction to Robotic Orthopaedics
Robotics has transformed modern orthopaedic surgery.
Offers precision, accuracy, and improved patient outcomes.
Used widely in joint replacement, spine surgery, trauma, and sports medicine.
2. Why Robotics? – Key Advantages
Greater surgical accuracy in implant positioning.
Real-time 3D planning for personalized surgery.
Reduced soft-tissue damage and minimal blood loss.
Faster recovery, shorter hospital stay, and early mobilization.
Increased implant longevity due to perfect alignment.
3. Applications in Orthopaedic Practice
Robotic-Assisted Knee Replacement – ensures perfect alignment and ligament balancing.
Robotic Hip Replacement – better cup placement, leg length correction, and stability.
Spine Robotics – accurate pedicle screw placement, reduced radiation exposure.
Trauma Surgeries – precision in complex fractures.
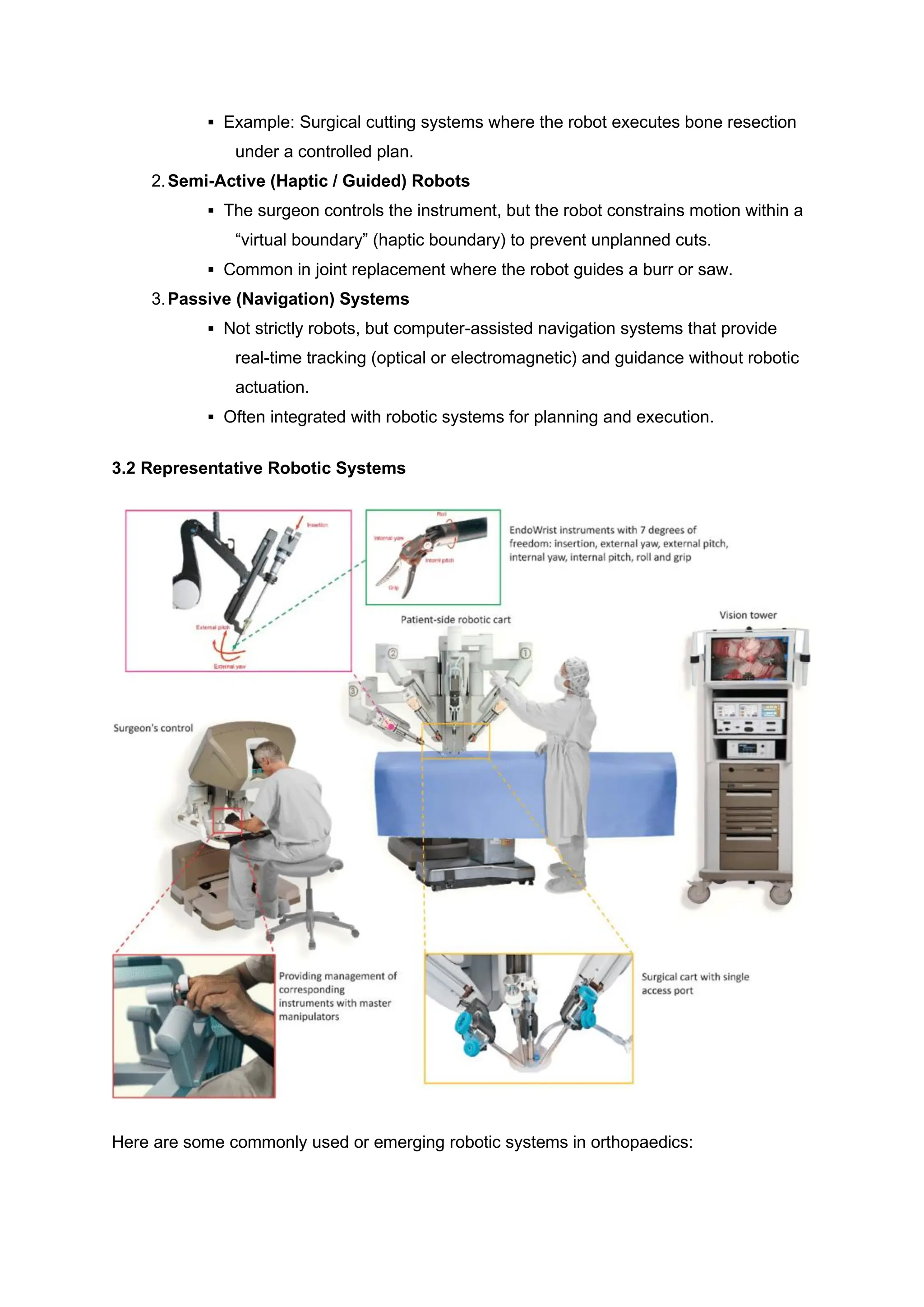
4. How the Robotic System Works
Pre-operative CT scan-based planning.
Surgeon-controlled robotic arm guides bone preparation.
Continuous intra-operative feedback ensures error-free cuts.
Surgeon remains in full control — robot enhances accuracy, not replaces the surgeon.
5. Patient Benefits
Smaller incision and minimal pain.
Faster return to routine activities.
Improved joint function and satisfaction.
Lower risk of revision surgery.
6. Future of Robotics in Orthopaedics
AI integration for predictive planning.
Fully automated surgical workflow.
Real-time analytics for even safer surgeries.