
Downloaded 373 times





























The document defines a health system as consisting of all organizations, people, and actions whose primary purpose is to promote, restore, or maintain health. It discusses health systems as complex adaptive systems with many interacting elements. It presents several conceptual frameworks for analyzing health systems, including the WHO health system building blocks and the Antwerp health system dynamics framework. It then discusses the concept of health system strengthening and changing global approaches to improving health systems over time, moving from a disease-focused approach to a more holistic health system strengthening approach.
The presentation introduces health systems, defines them, and outlines frameworks for strengthening.
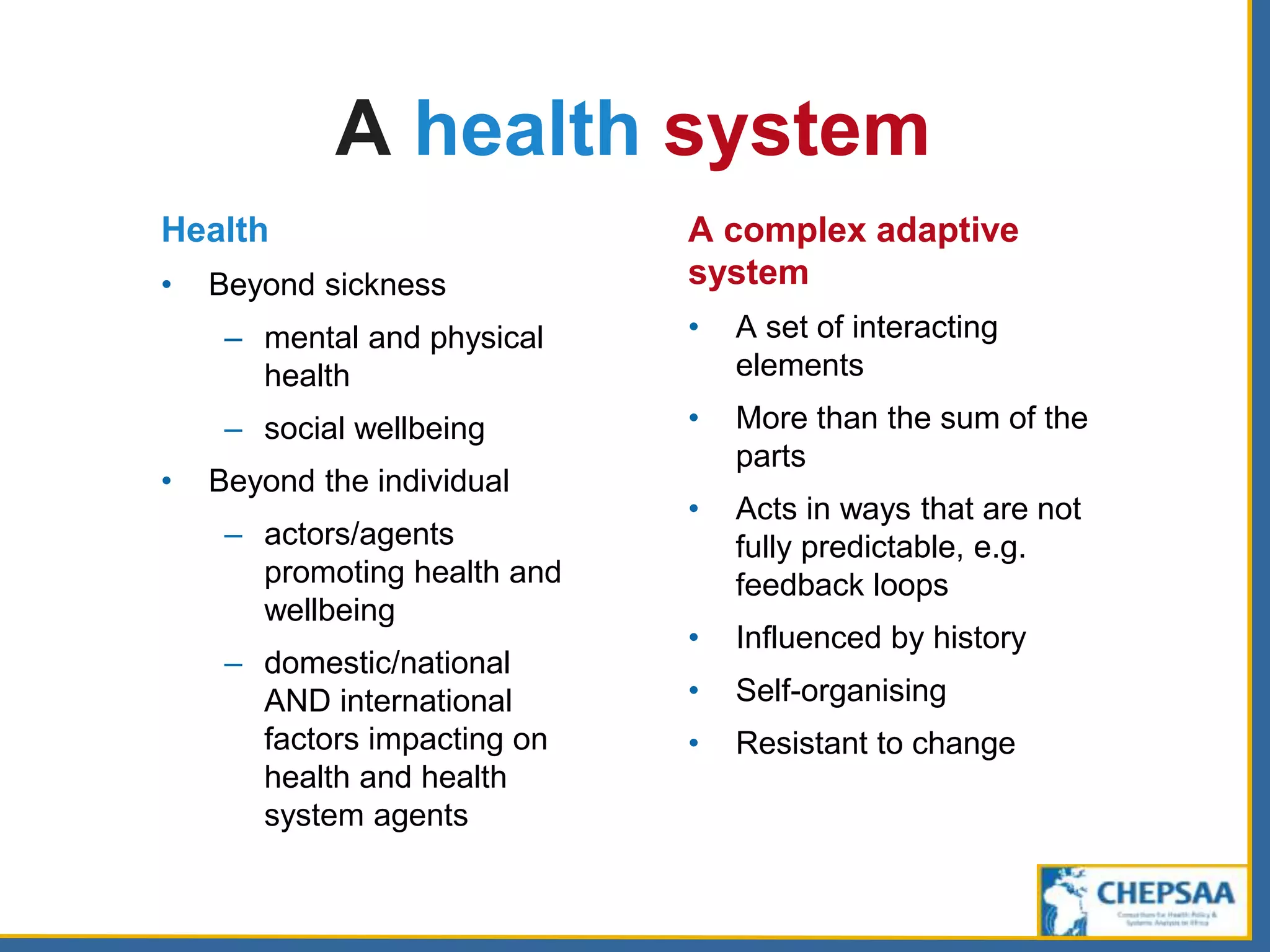
According to WHO, health systems consist of all entities promoting health, functioning as complex adaptive systems.
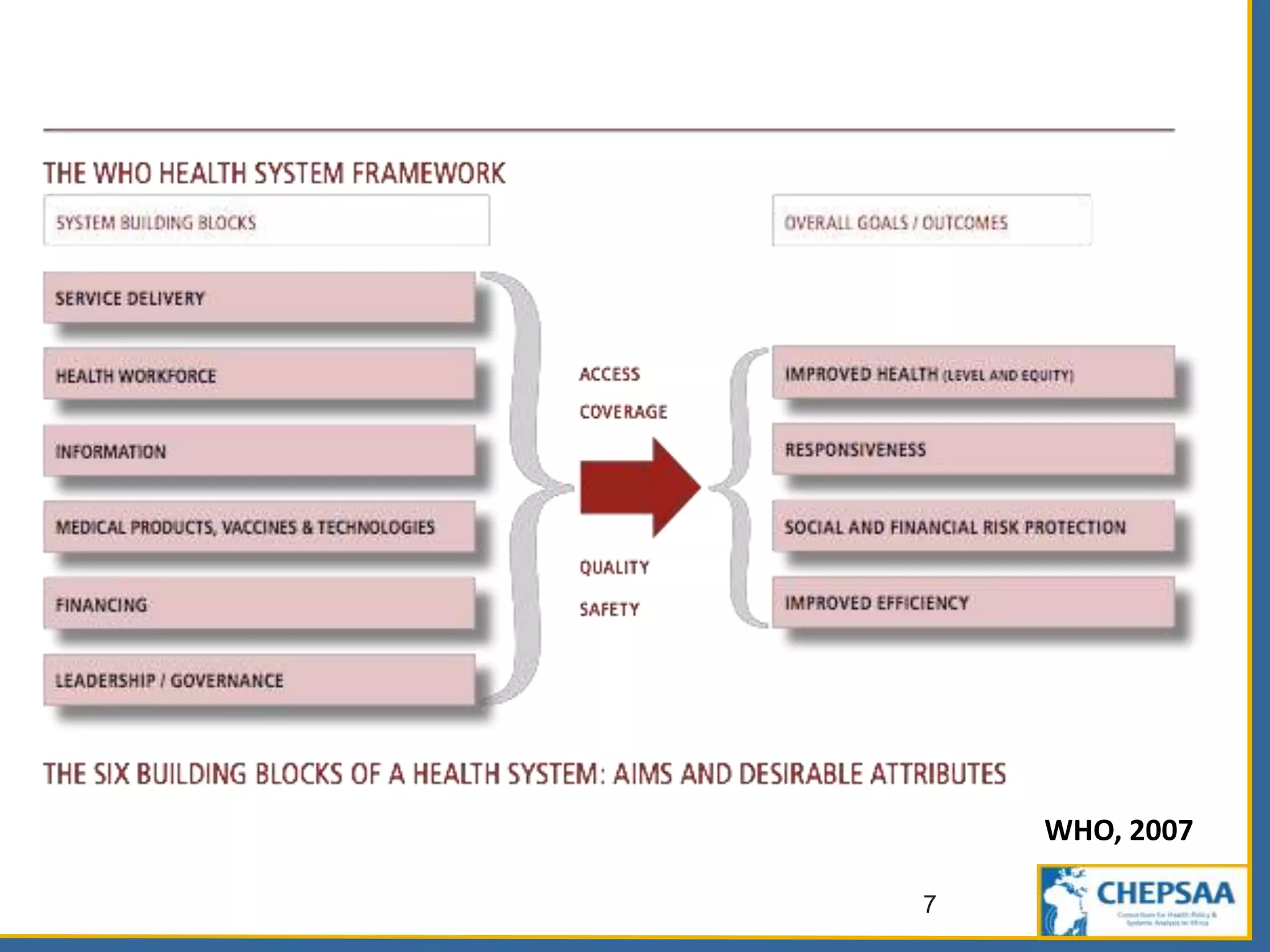
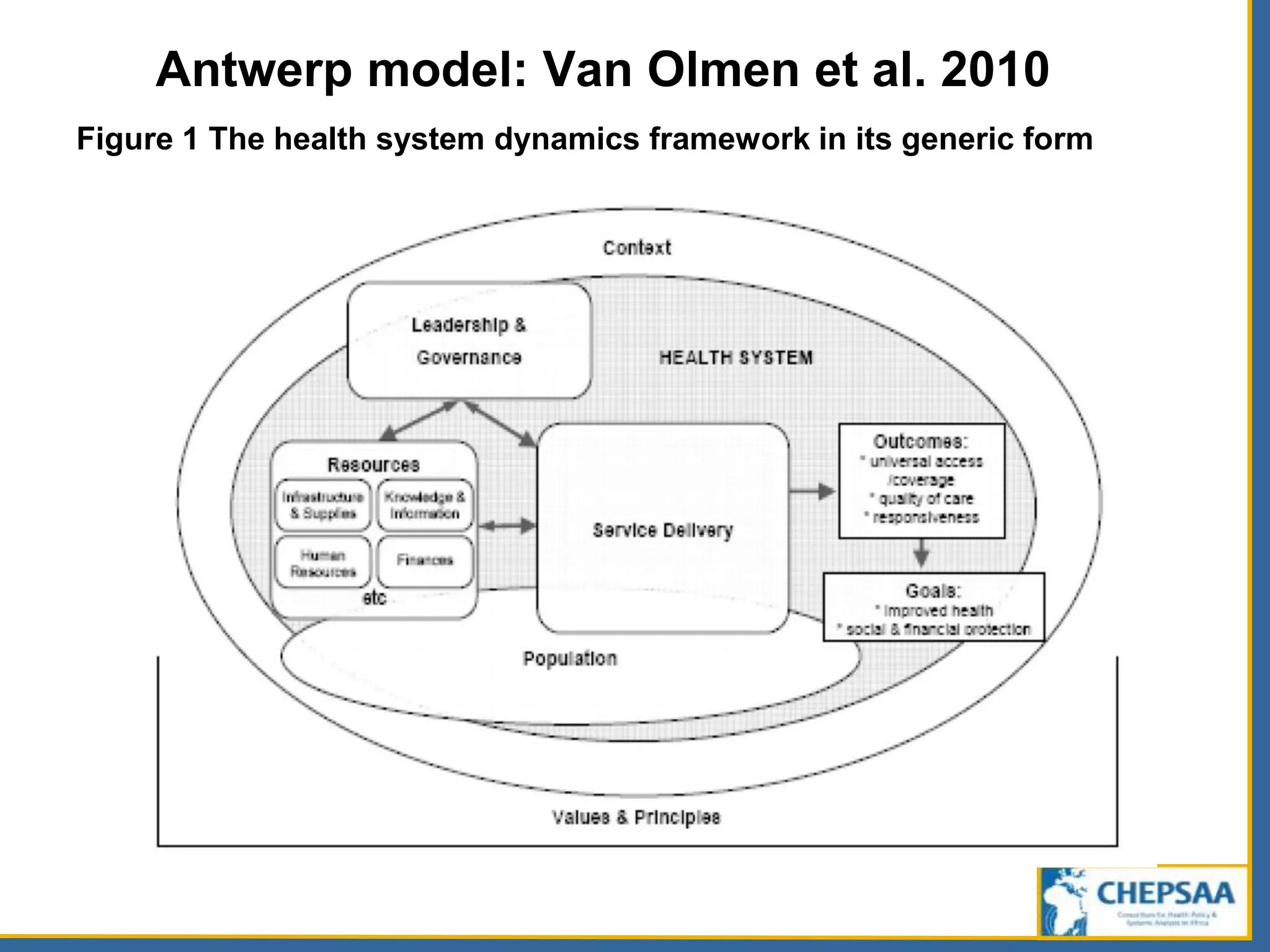
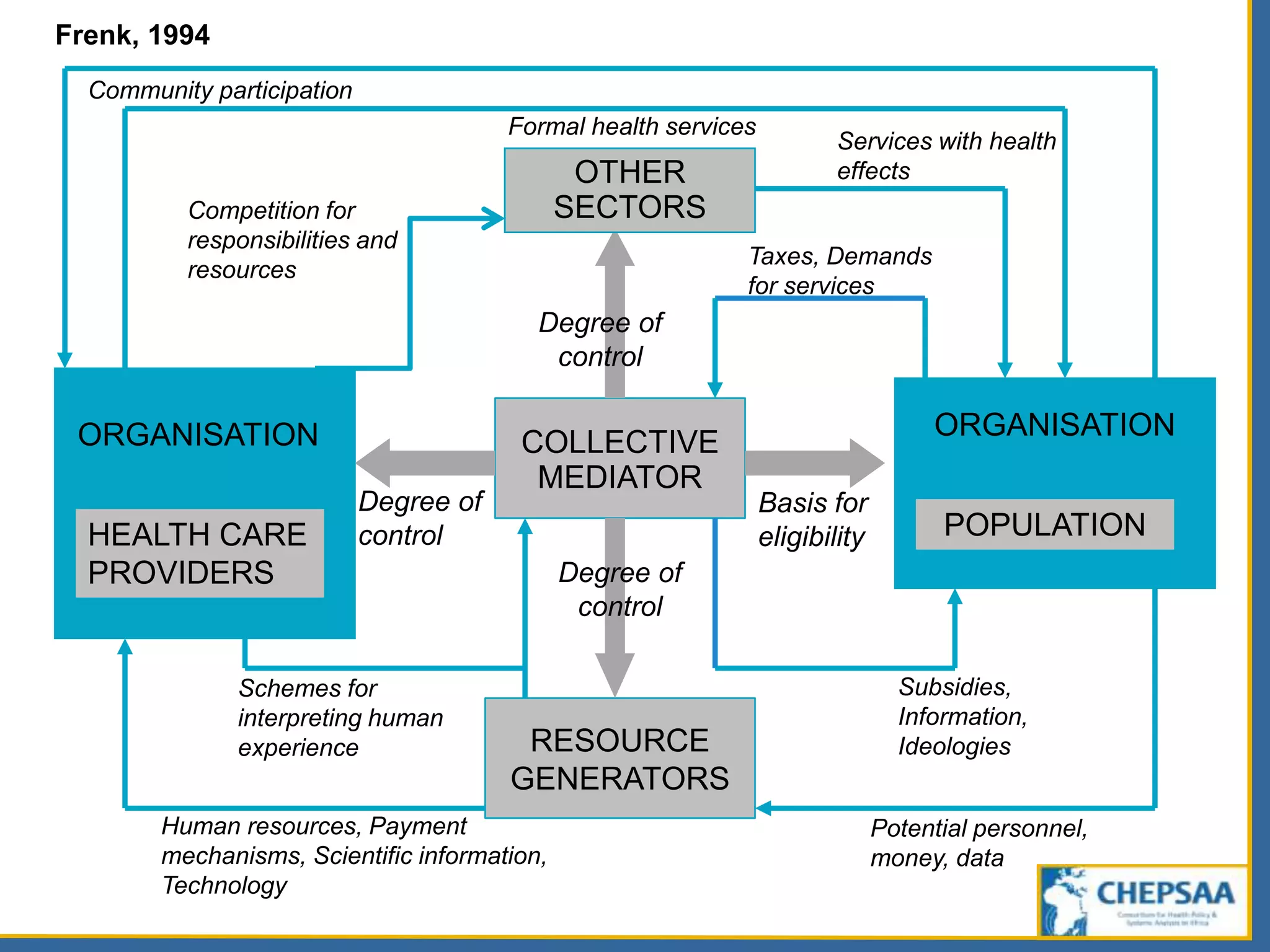
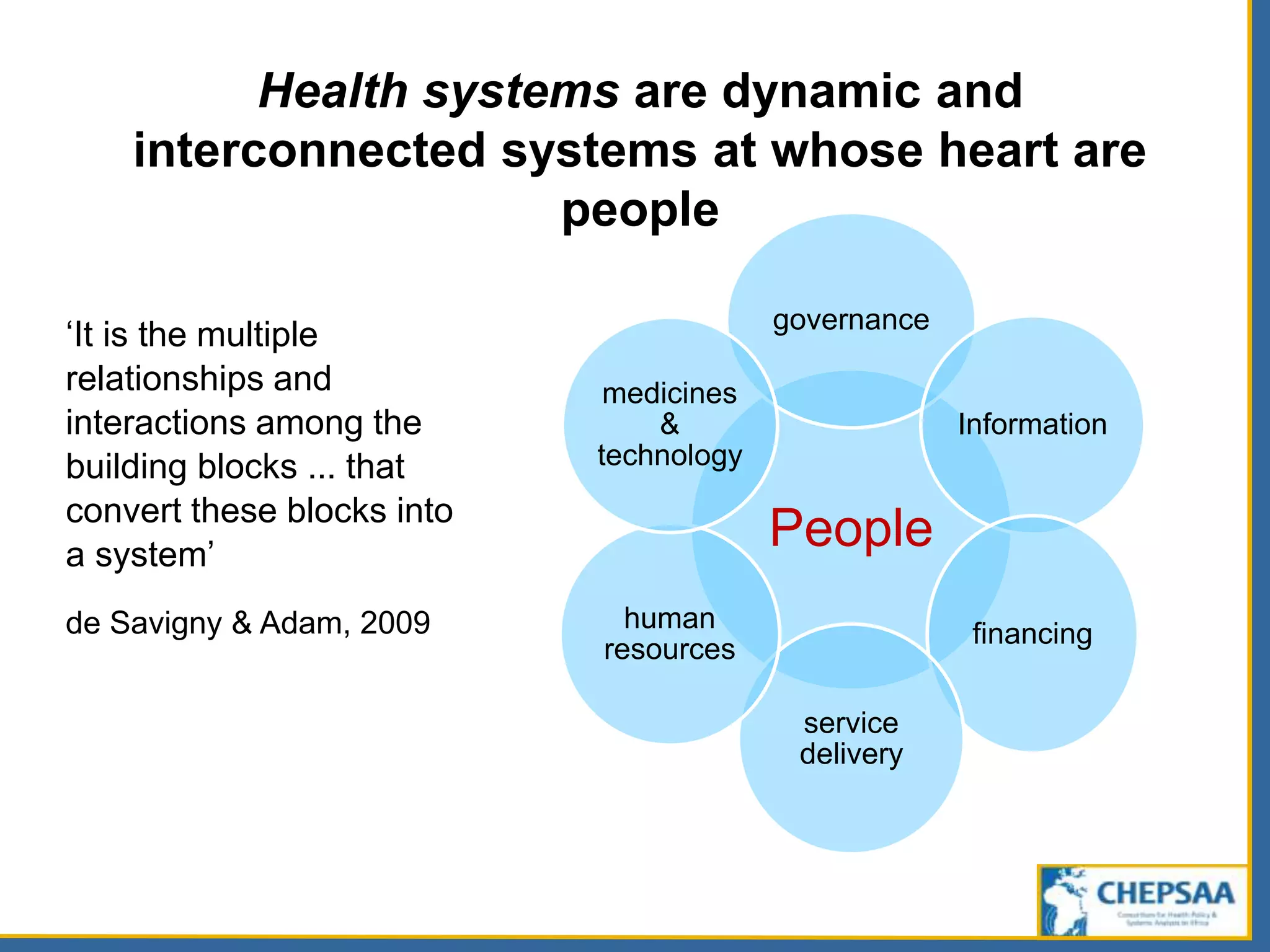
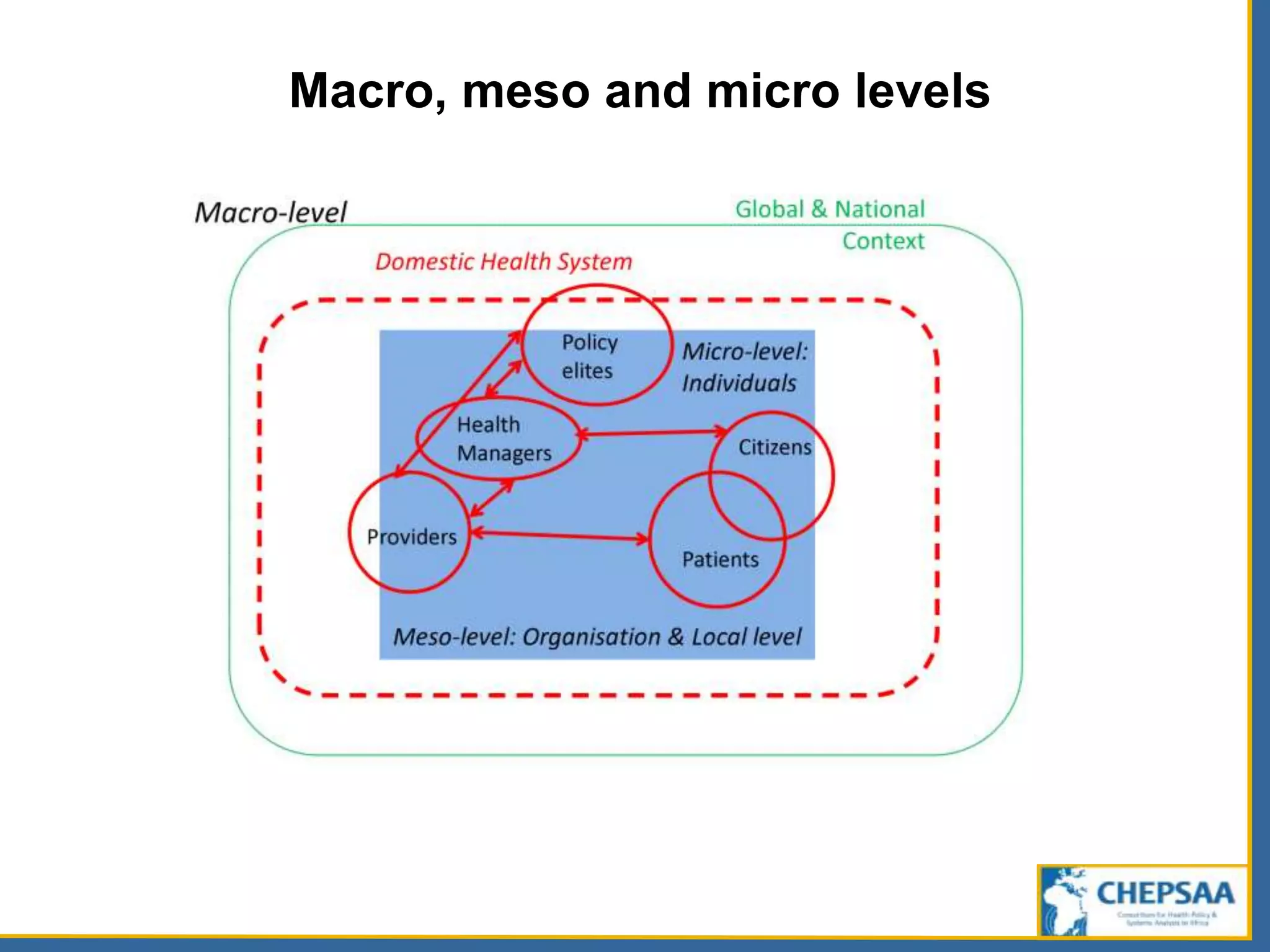
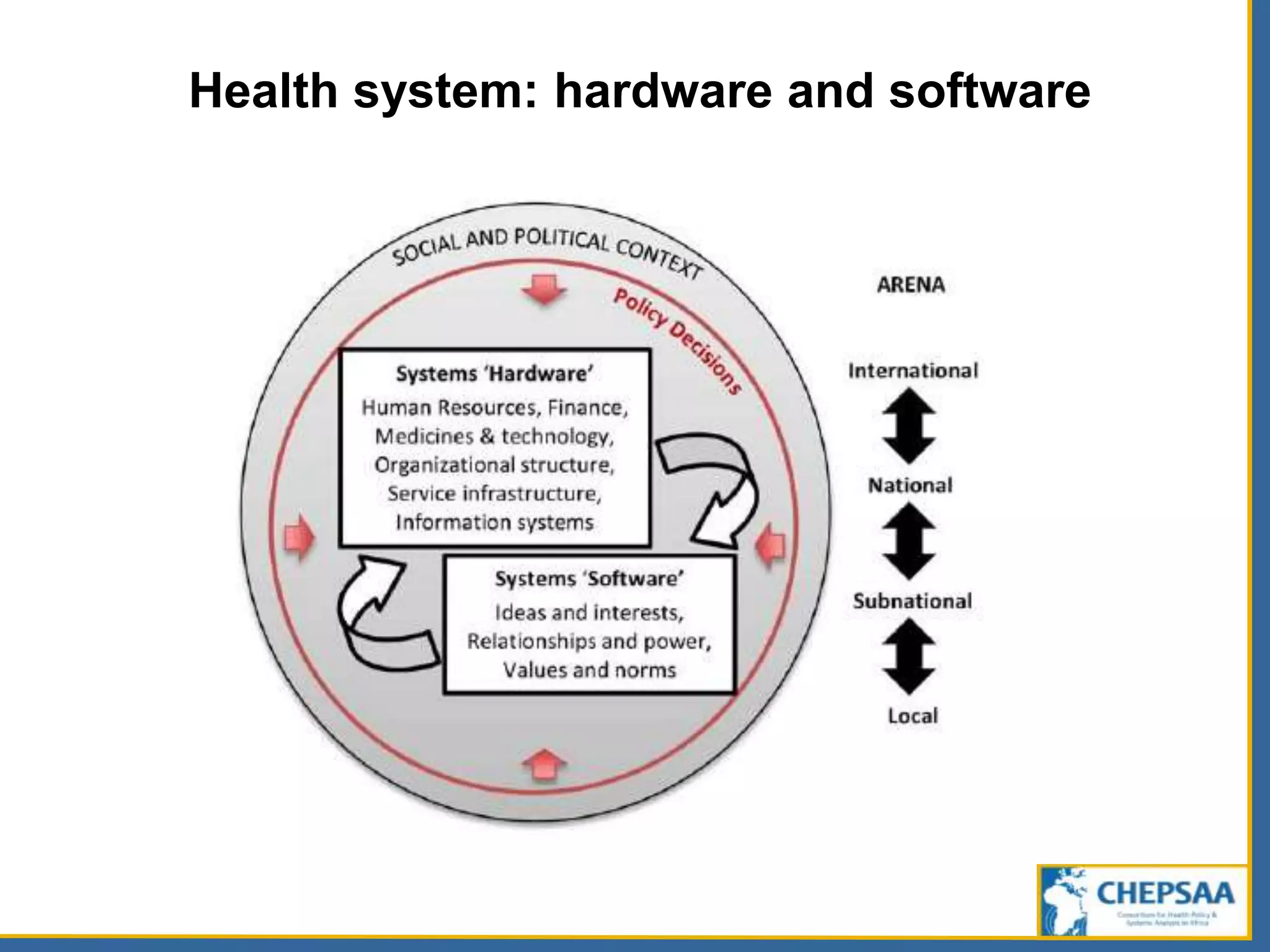
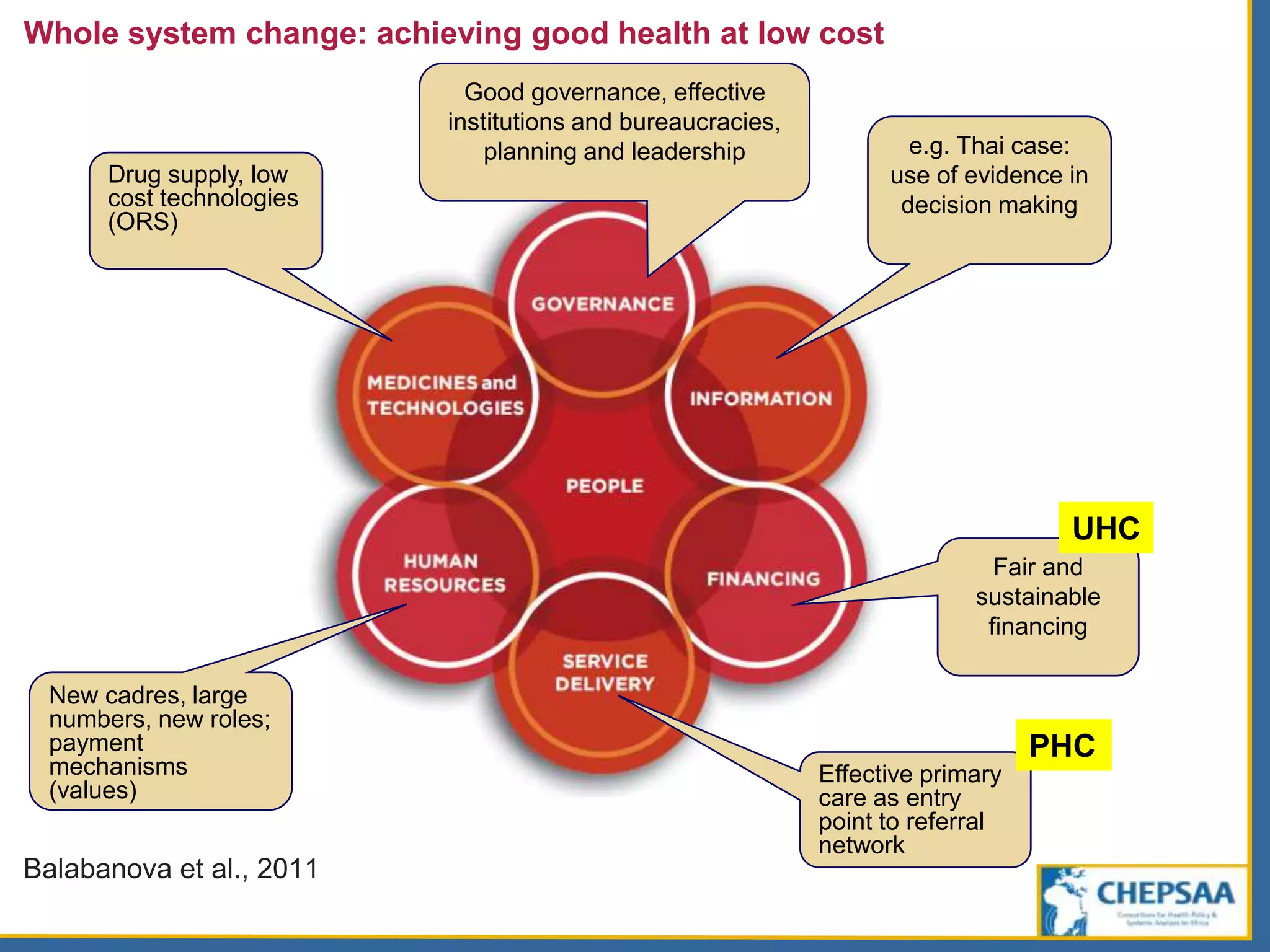
Discusses various frameworks that illustrate the interactions within health systems, emphasizing governance and people.
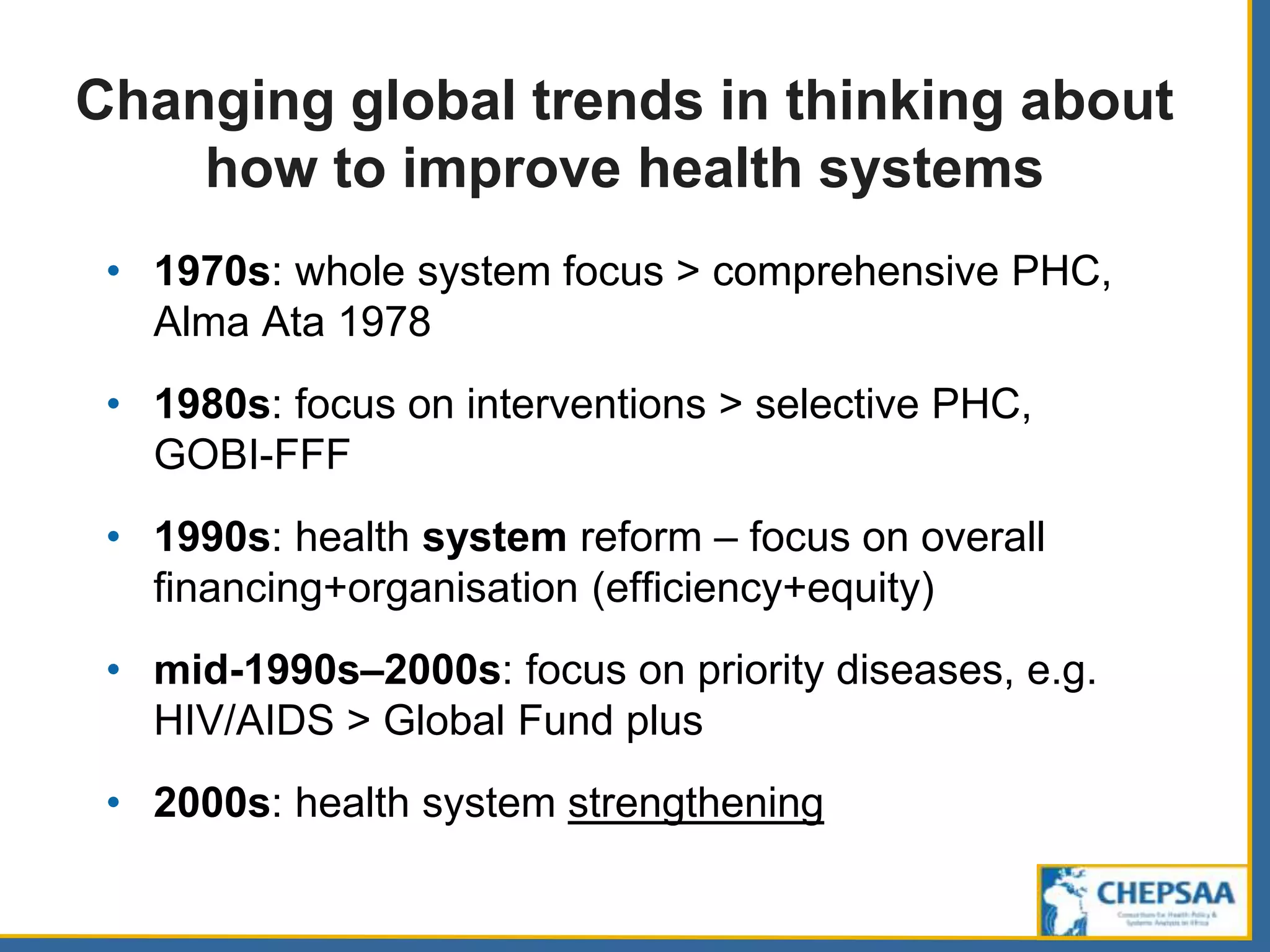
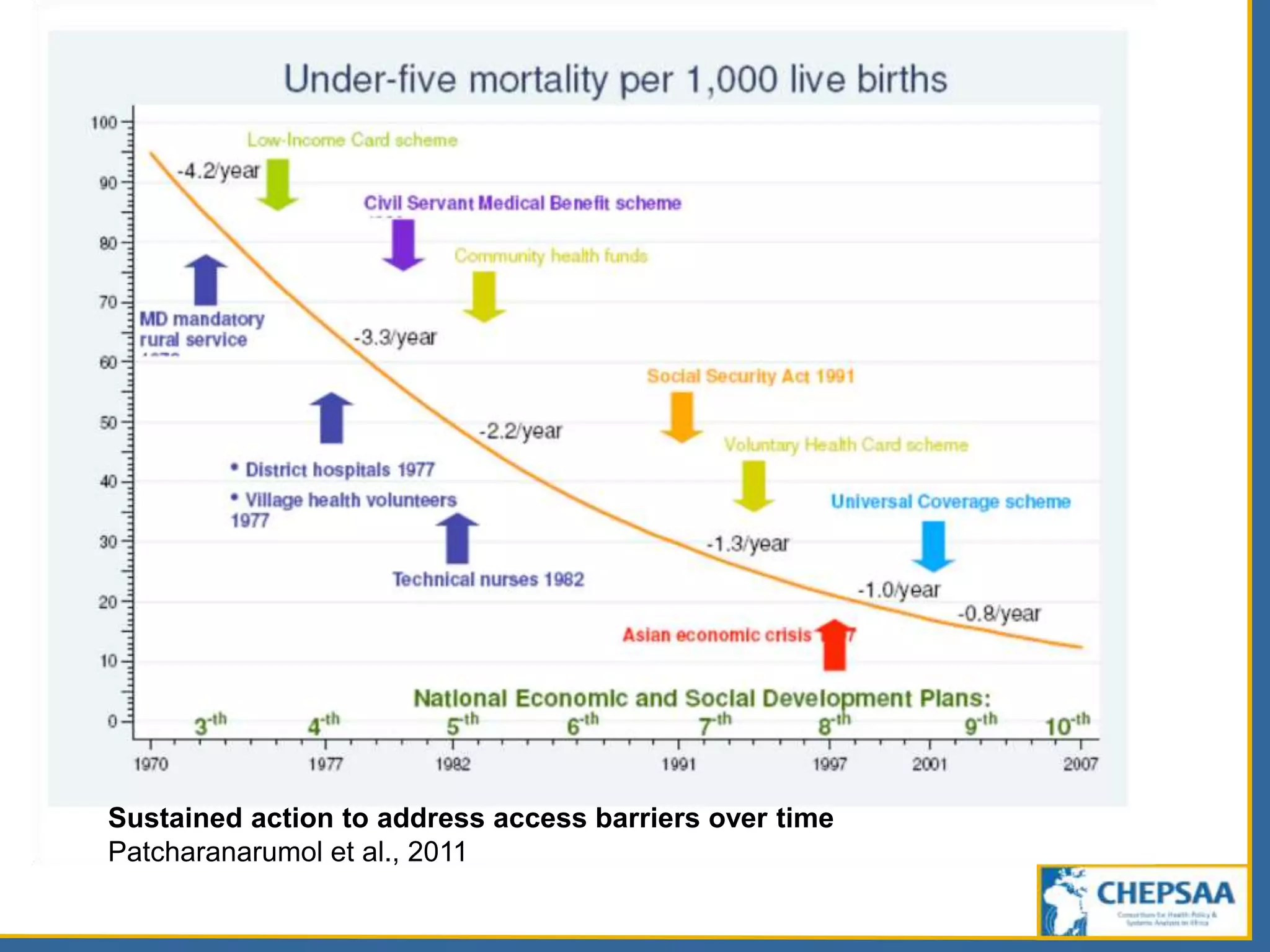
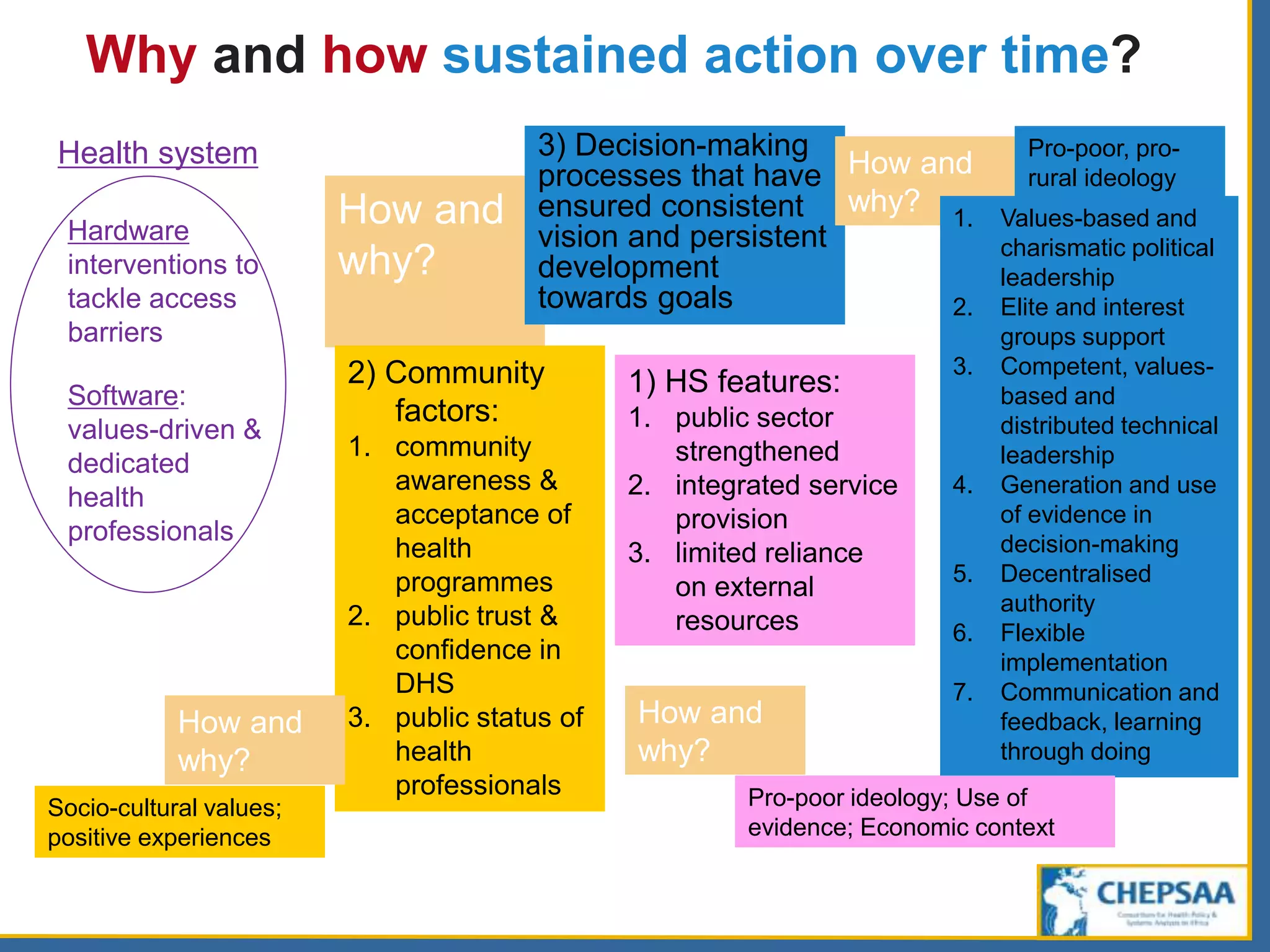
Traces evolution of global health focus since the 1970s towards comprehensive health system strengthening.
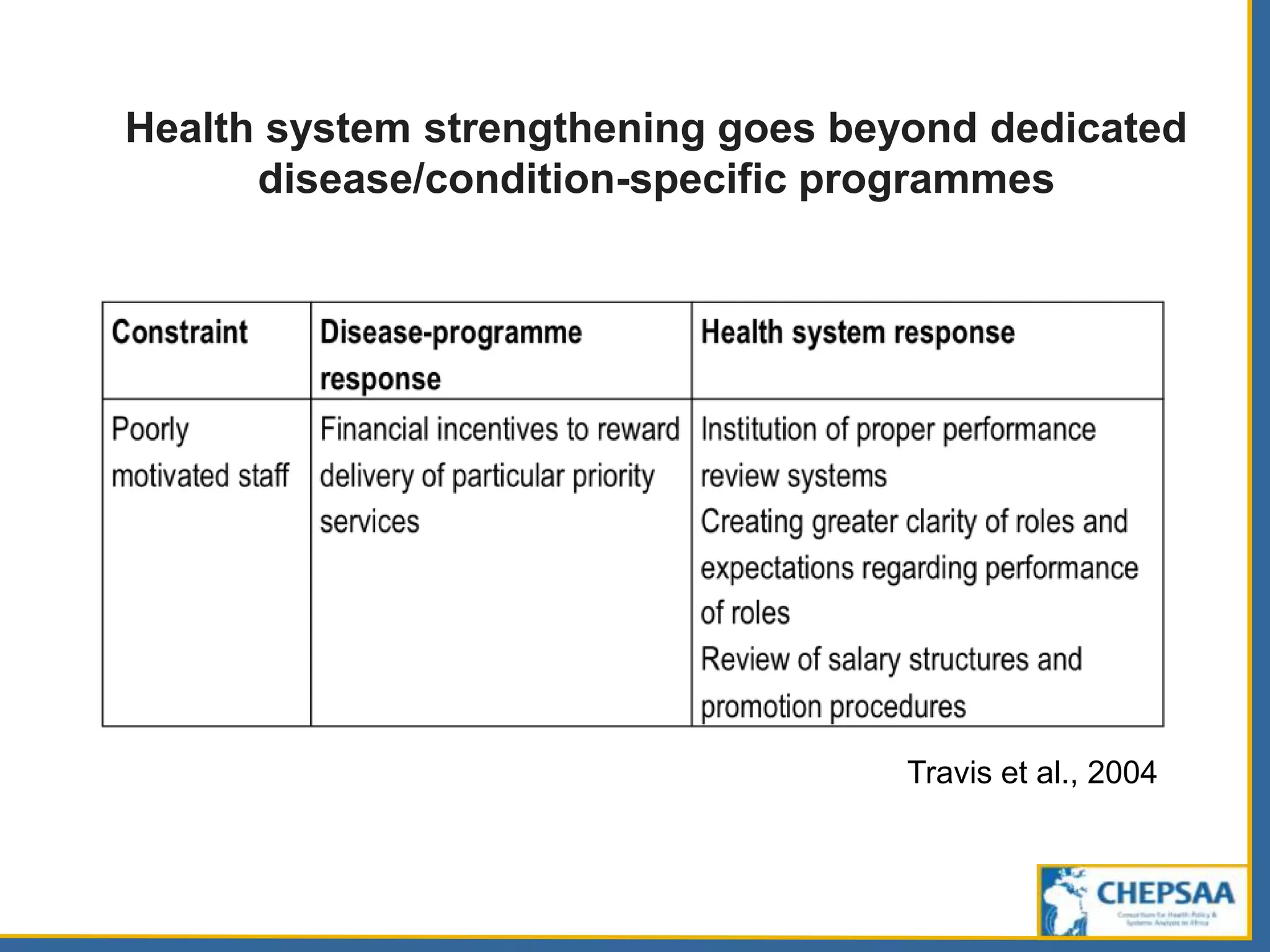
Highlights the need for holistic approaches beyond disease-specific programs, using successful case studies.
Explains health policies as crucial actions to enhance health system performance but warns of political complexities.
Mentions partnerships across academic institutions for health policy and systems research, promoting shared goals.










































































![Rheumatic Fever CASE PRESENTATION [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationautosaved-251123182512-9d9b0da4-thumbnail.jpg?width=640&height=640&fit=bounds)











