Download to read offline
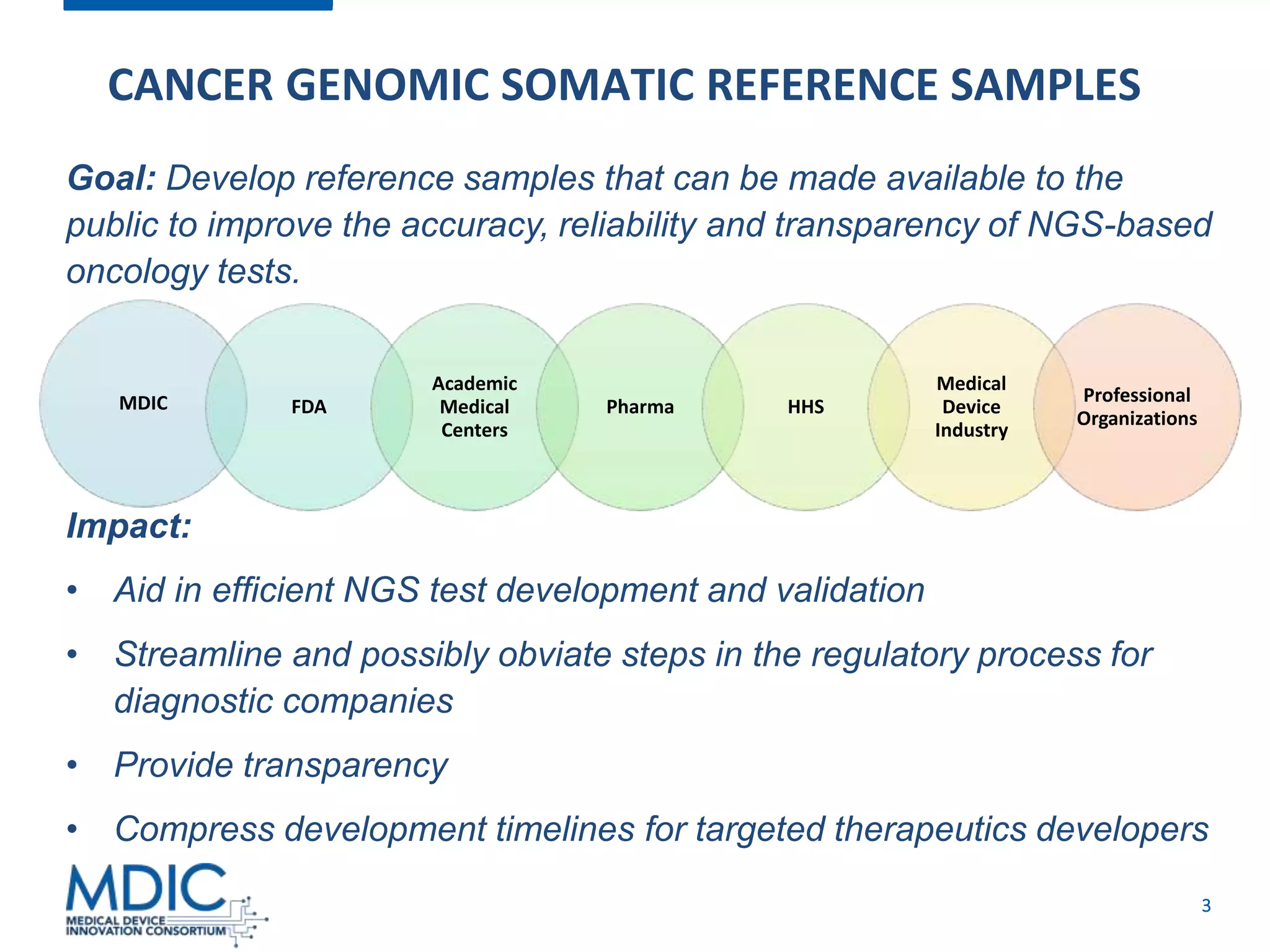
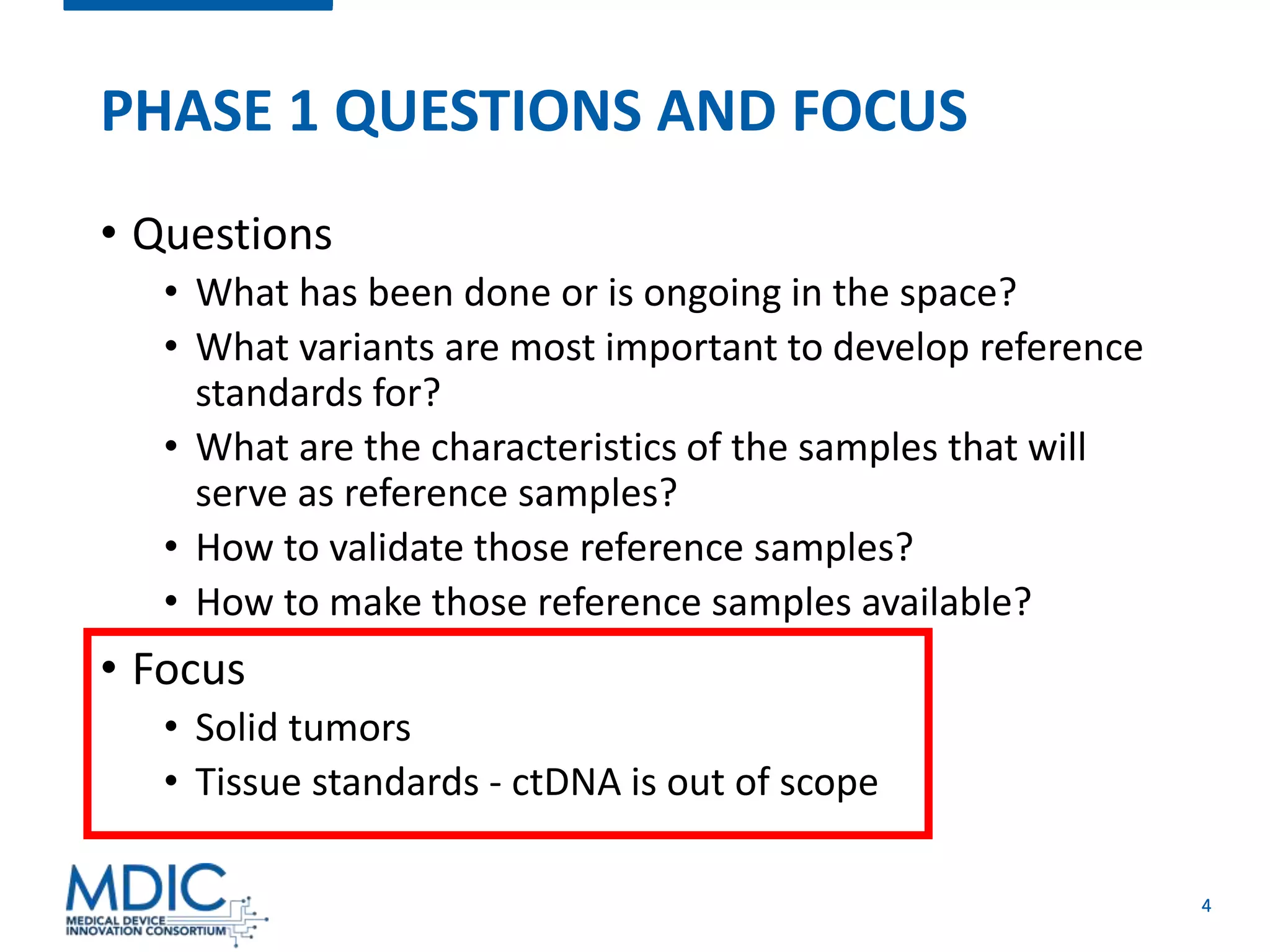
























This document provides an overview of the Cancer Genomic Somatic Reference Samples initiative, a collaborative effort to develop reference samples to improve next-generation sequencing (NGS) cancer tests. The initiative is working in phases to prioritize clinically relevant variants, analyze existing reference material efforts, define desired sample characteristics, and issue requests for information and proposals. The goal is to make reference samples available publicly to help diagnostic companies validate NGS tests and streamline regulatory processes, providing transparency. Upcoming webinars will focus on selecting tumor suppressor genes and genomic signatures for inclusion.























































































