This document discusses different types of version procedures used to change the fetal position in the uterus. It describes external cephalic version, internal podalic version, and bipolar version. External cephalic version involves manually turning the fetus from breech or transverse position to head-down position. Internal podalic version is only used for transverse lie twins and involves manually delivering one or both feet of the breech fetus. Bipolar version corrects transverse lie in a dead or premature fetus by manipulating the fetus both internally and externally. The document provides details on indications, contraindications, procedures and complications for each version type.
DEFINITION
Version isthe turning out of fetus from one
presentation to another and may be done either
externally or internally by the physician.
If the aim is to make the head the presenting part is
called cephalic version and if the breech will be the
presenting part it is called podalic version.
3.
TYPES OF VERSION
According to the methods employed.
1. External cephalic version
2. Internal podalic version
3. Bipolar version
4.
External cephalic version
It is a procedure used to turn a fetus from a breech
position or transverse position into a cephalic pole of
the uterus.
PRELIMINARIES
The patientis asked to empty bladder.
She is to lie on her back with the sholders slightly
raised and the thighs slightly flexed.
abdomen is fully exposed and FHR is auscultated.
The most commonly used tocolytic medication
(terbutaline-0.25mg sc.) Because of uterus is
relaxed.
7.
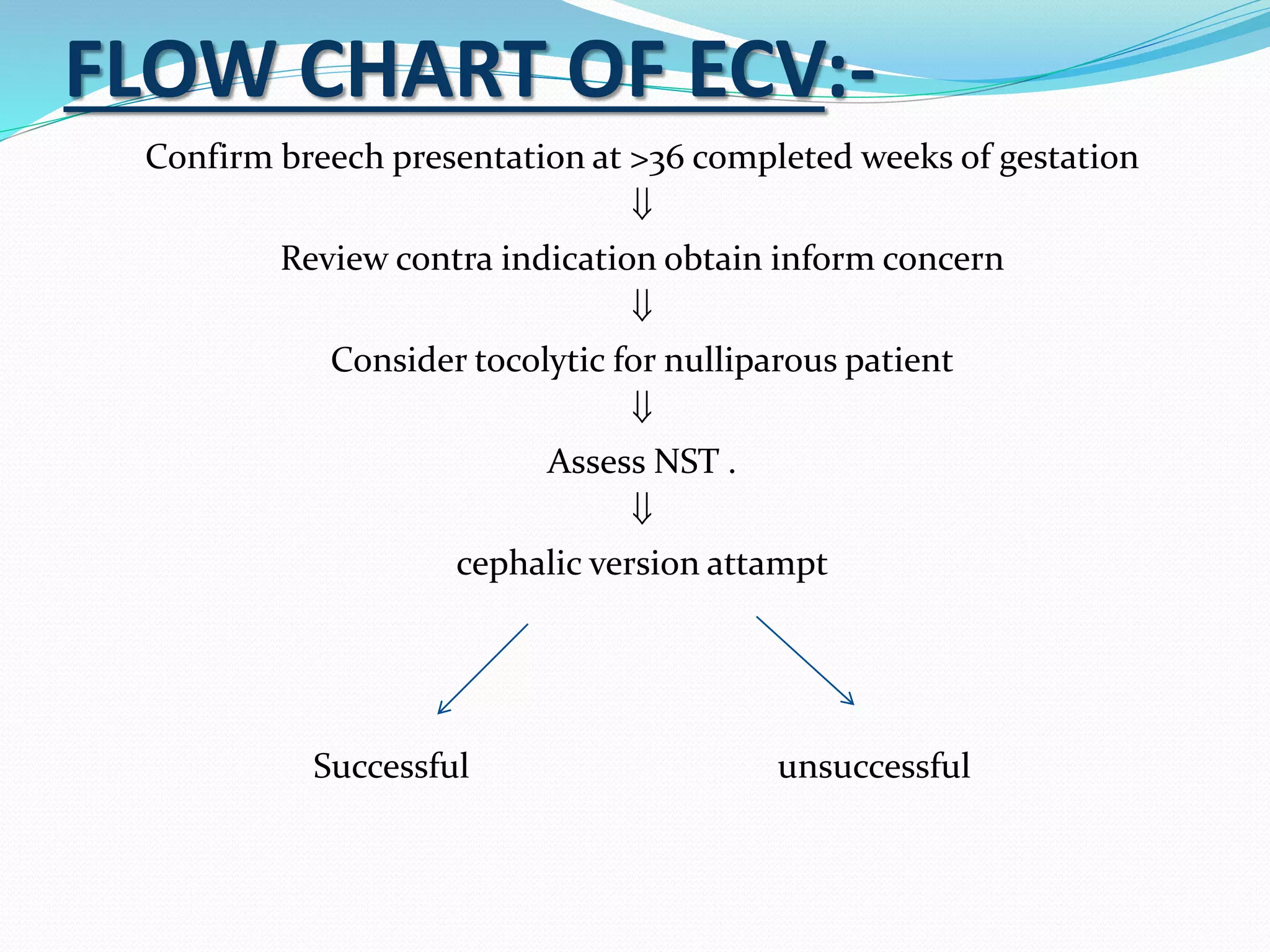
FLOW CHART OFECV:-
Confirm breech presentation at >36 completed weeks of gestation
Review contra indication obtain inform concern
Consider tocolytic for nulliparous patient
Assess NST .
cephalic version attampt
Successful unsuccessful
8.
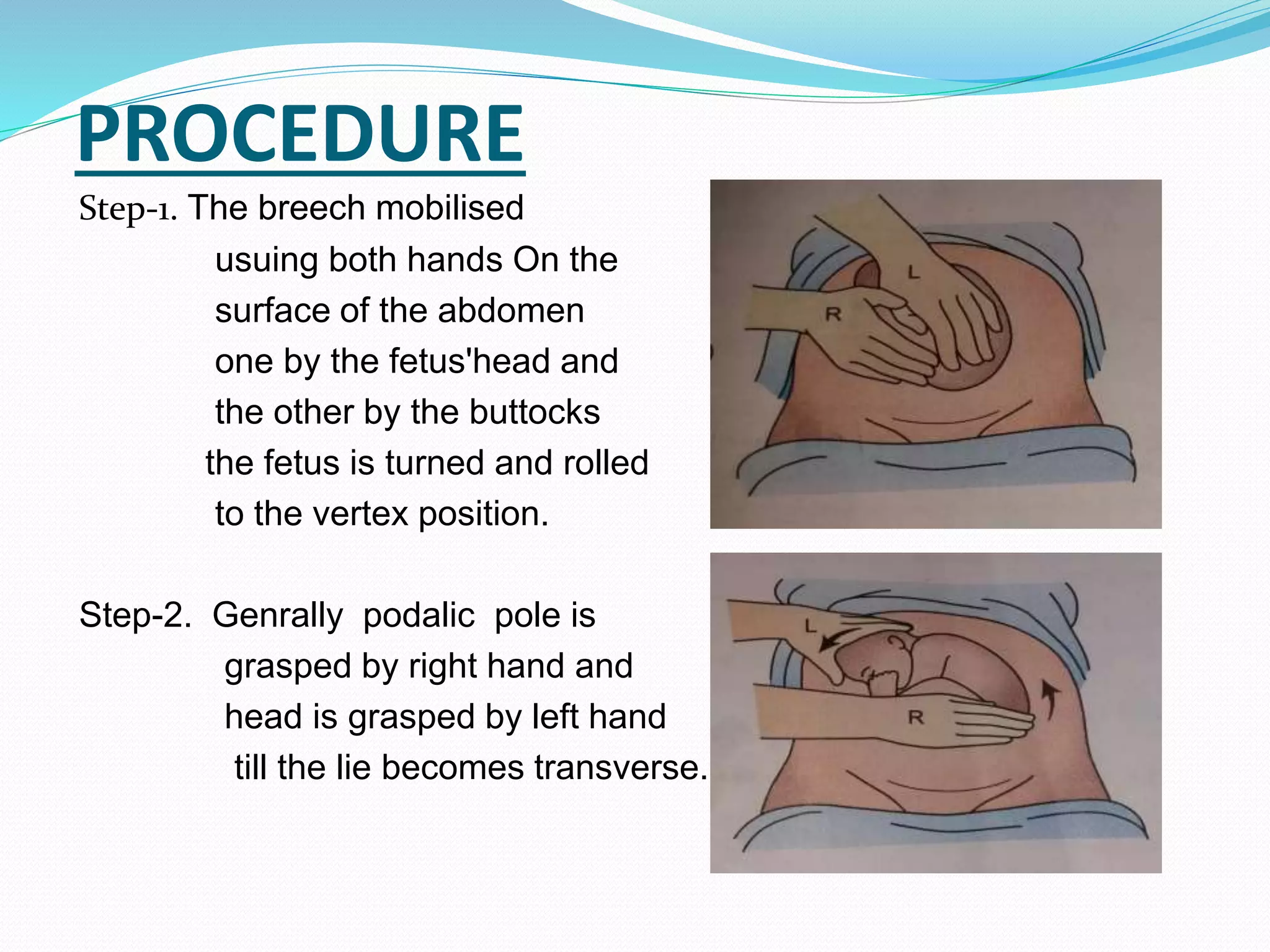
PROCEDURE
Step-1. The breechmobilised
usuing both hands On the
surface of the abdomen
one by the fetus'head and
the other by the buttocks (a) (a)
the fetus is turned and rolled
to the vertex position.
Step-2. Genrally podalic pole is
grasped by right hand and
head is grasped by left hand (b) (b)
till the lie becomes transverse.
9.
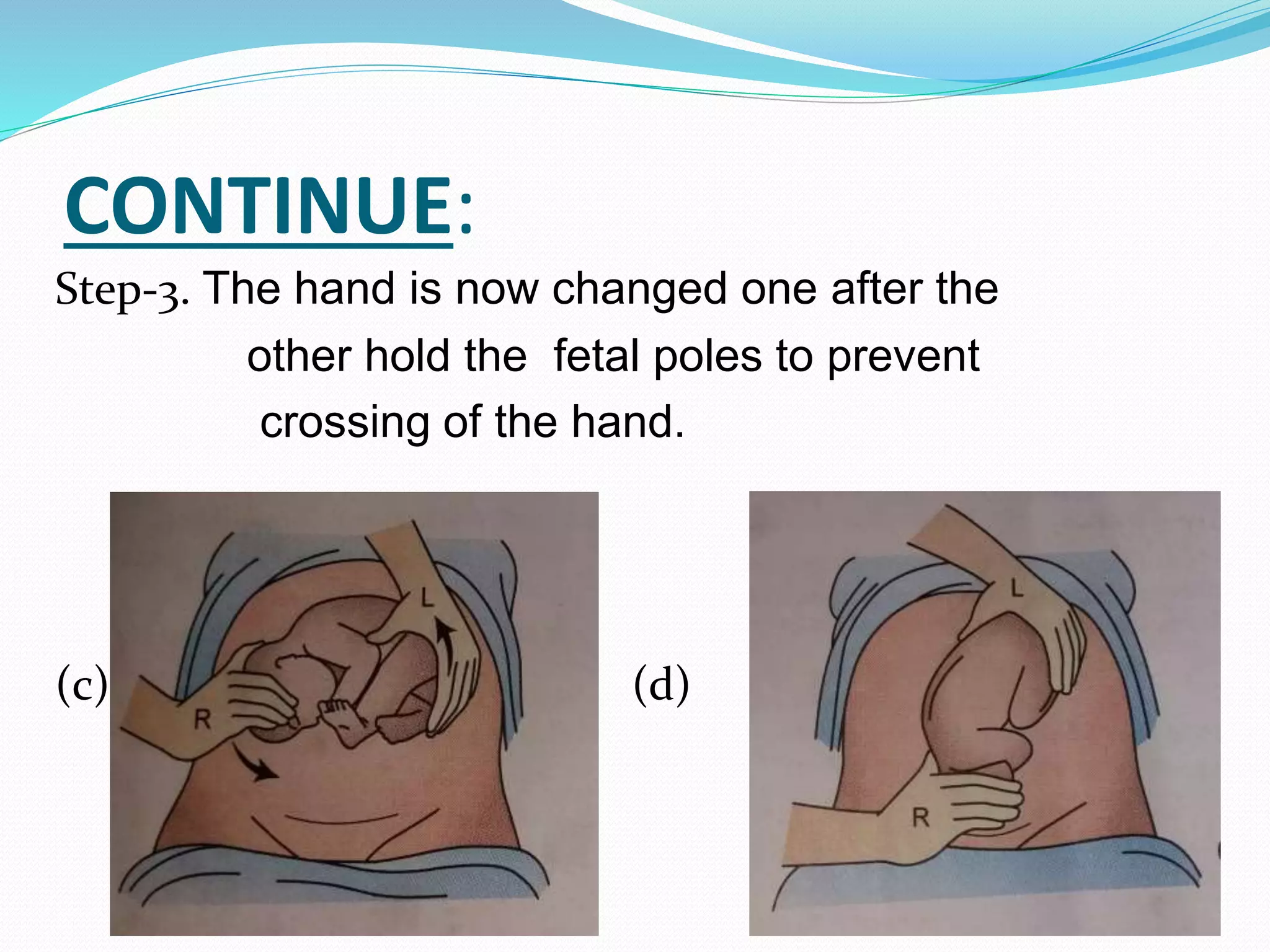
CONTINUE:
Step-3. The handis now changed one after the
other hold the fetal poles to prevent
crossing of the hand.
(c) ( (d)
10.
INSTRUCTIONS
The patient isadvised for follow up to check the
corrected position.
To report to the physician if there is vaginal bleeding
or liquor amnii.
Rh-negative non immunised women must be
protected by intramuscular administration of 100.mug
anti-D gamma globulin.
11.
CONTRAINDICATION
Fetal distress.
The amniotic sac has ruptured.
A mother has a condition(such a heart problem).
A ceaesarean delivery is needed,such as when there
is placenta praevia or abruptio placentae.
12.
Advantages of ECV
1.Reduces the number of caesarean delivery.
2. Reduces maternal morbidity due to caesarean or
vaginal breech delivery .
3. Reduces the fetal hazards of vaginal breech
delivery.
13.
INTERNAL PODALIC VERSION
Internalversion is always a podalic version and is
almost always completed with the extraction of the
uterus.
14.
INDAICATION
Its only indicationbeing the transverse lie in case of
the second baby of twins.
However, it may be employed in singleton pregnancy
to expedite delivery in adverse condition where the
caesarean section facilities are lacking. Such condition
are:
1. Transverse lie with cervix fully dilated.
2. Cord prolapse with cervix fully dilated with
transverse lie or head high up and the baby is alive.
15.
PRELIMINARIES
1. Lithotomy position.
2.Empty bladder.
3. Given general anesthesia.
4. Antiseptic cleaning draping and catheterisation are
done.
5. Wearing gloves.
16.
PROCEDURES
Step-1: If thepodalic pole of the fetus is on left side of
the mother, the right hand is to be introduced and vice
versa.
Step-2: The identification of the foot is done by
palpation of the heel.
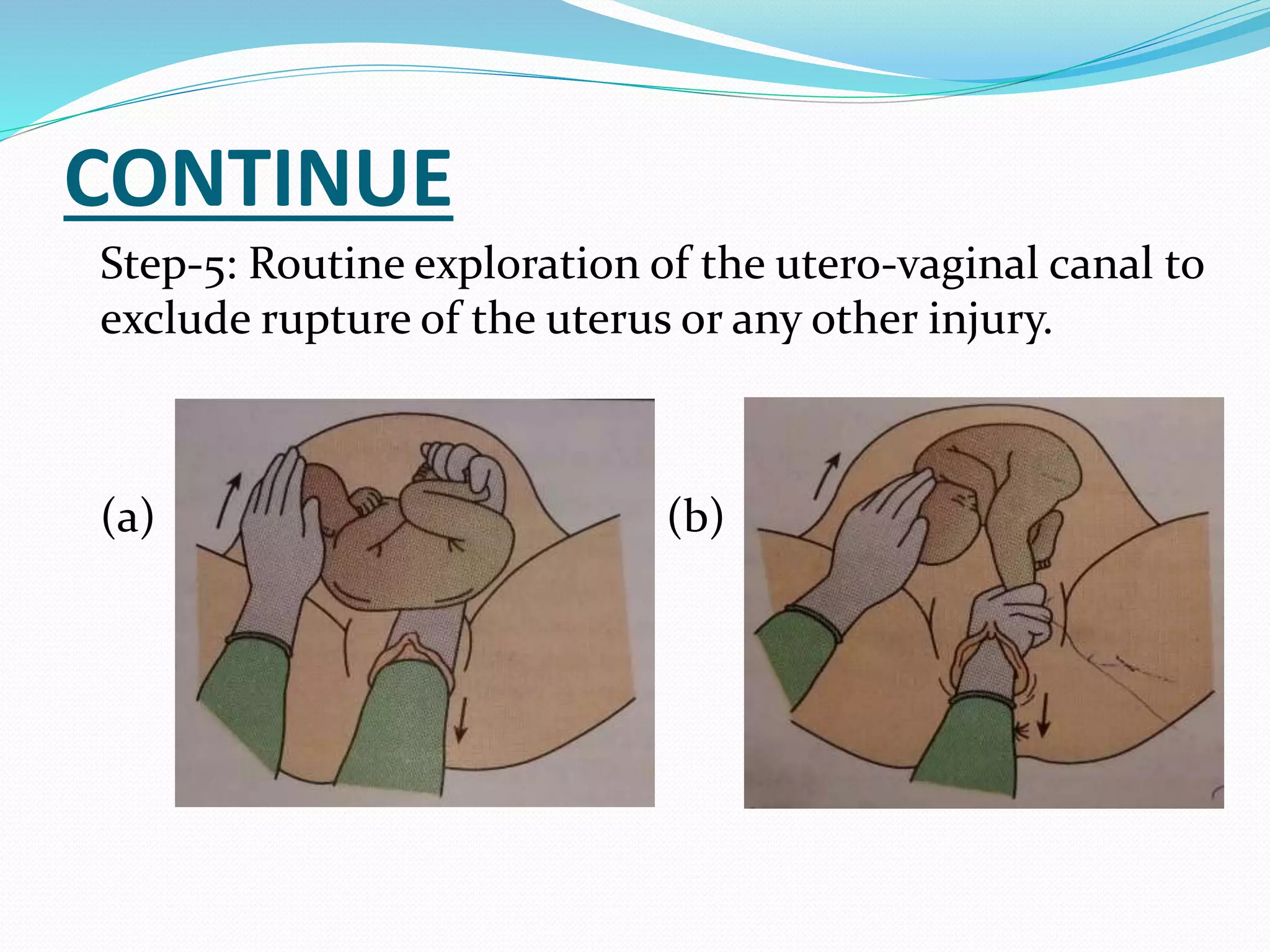
Step-3: While the leg is brought down by a steady
traction the cephalic pole is pushed up using the
external hand.
Step-4: After one leg is brought down,there is no
difficulty to deliver the other leg.
COMPLICATIONS
Maternal risk include-
1. Placental abruption.
2. Rupture of the uterus.
Fetal risk include -
1. Asphyxia.
2. Cord prolapse.
3. Intra cranial hemorrhage.
20.
BIPOLAR VERSION
It alsoknown as braxton-hicks. The conversation is done
introducing one or two finger through the cervix and the
other hand on the abdomen.
PROCEDURE
Under thepulled through general anethesia.
At least two finger are passed through the partially
dialated cervix, the foot is grasped as in internal
podalic version pulled through the cervix while the
other hand is assisting the version extrernally .
23.
CONCLUSION
First Iwould like to thank mrs. Snehalata parashar
madam who guided me and all 4th year students who
co-operated. As about discuss topic version
definition, types, and discription .
24.
BIBLIOGRAPHY
BOOK REFFERANCE
1. AnnamaJocab, text book of comprehensive text
book of ‘MIDWIFY and GYNECOLOGY nursing ‘
JAYPEE publication 3rd edition page no.285-287.
2. D.C. DUTTA text book of obsterical including
perinatary and contraception central publication 7th
edition page no. 583-585.
3. NET REFFERANCE
www.wikipedia.com
www.pubmad.com