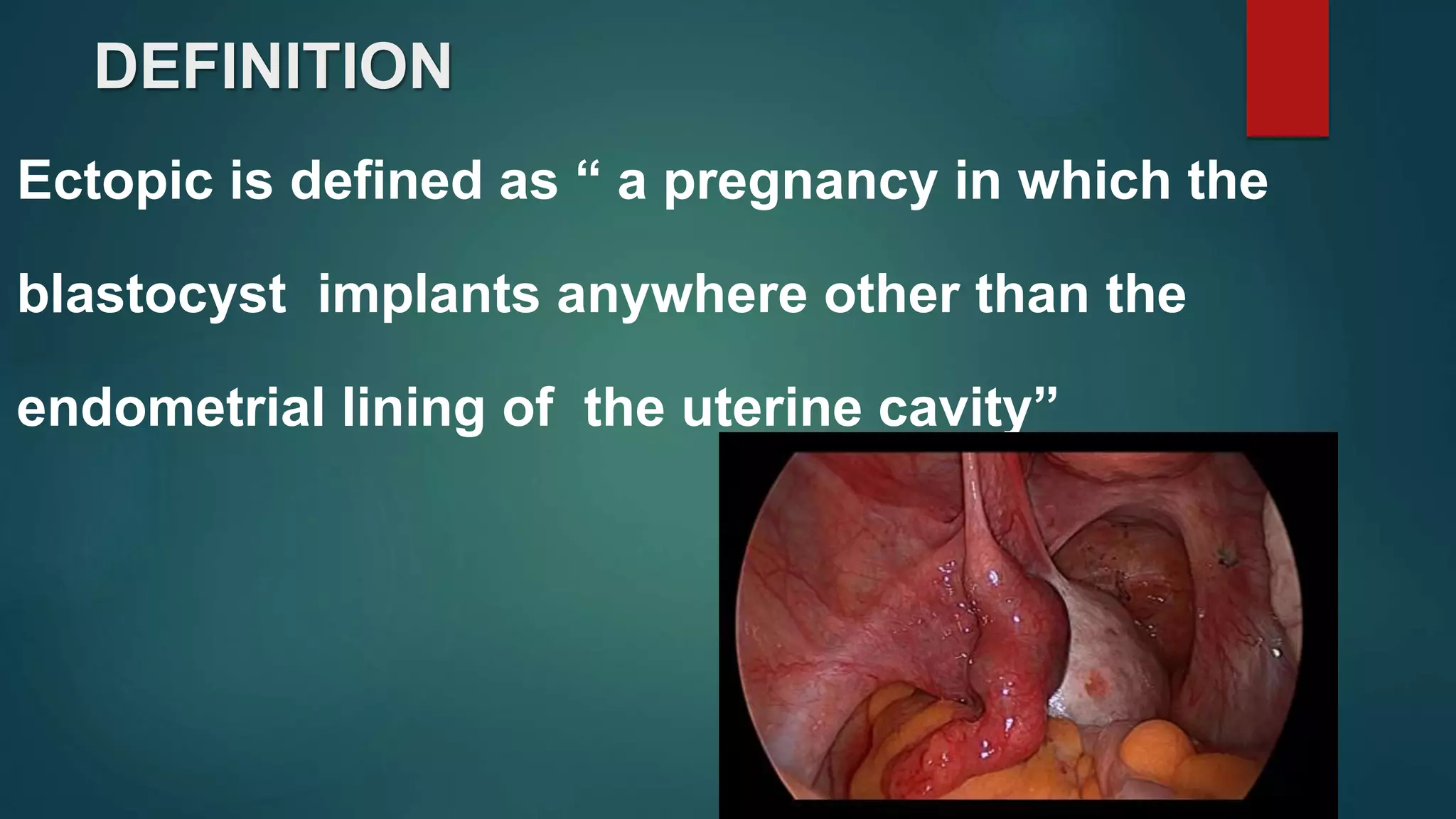
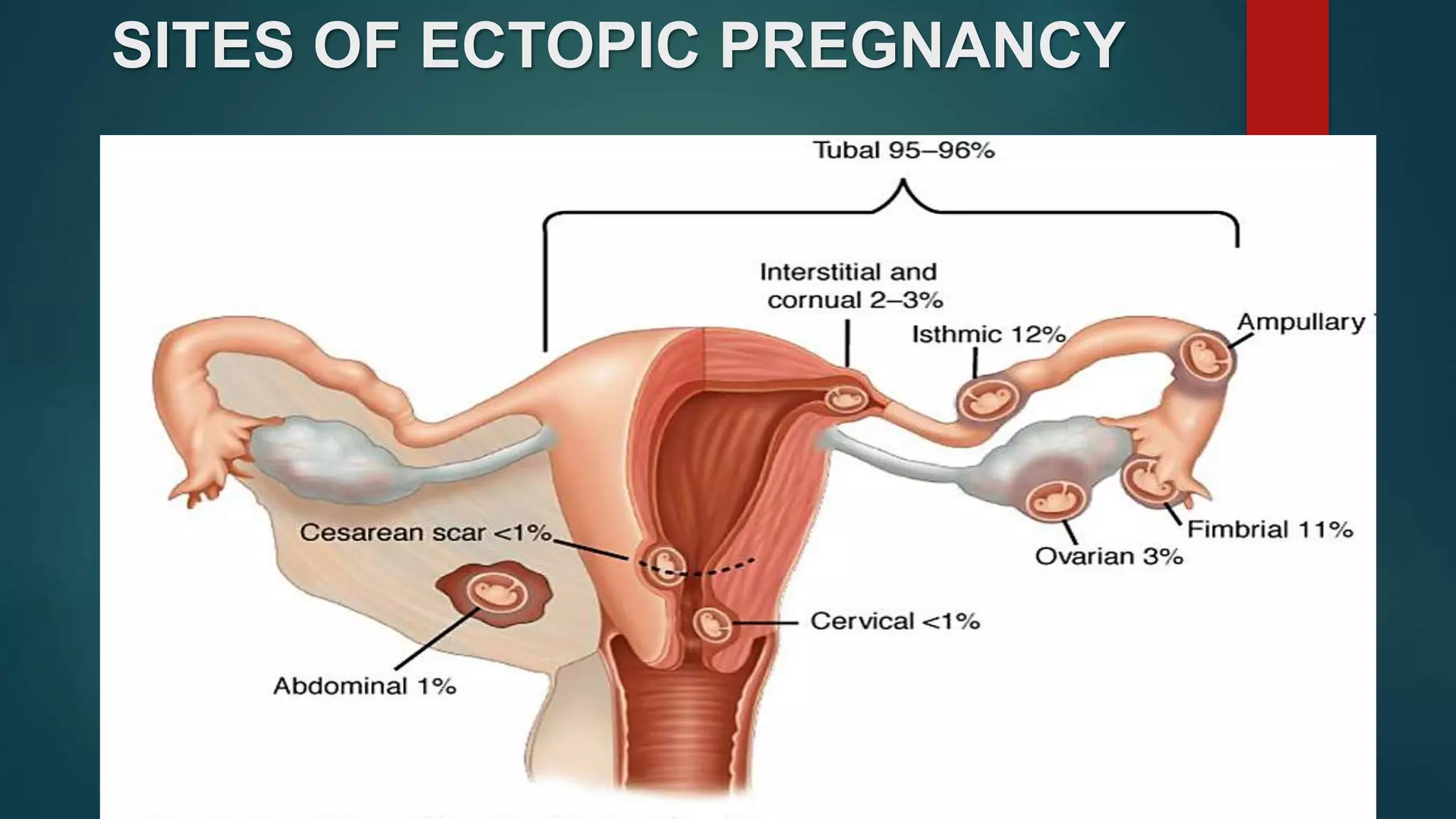
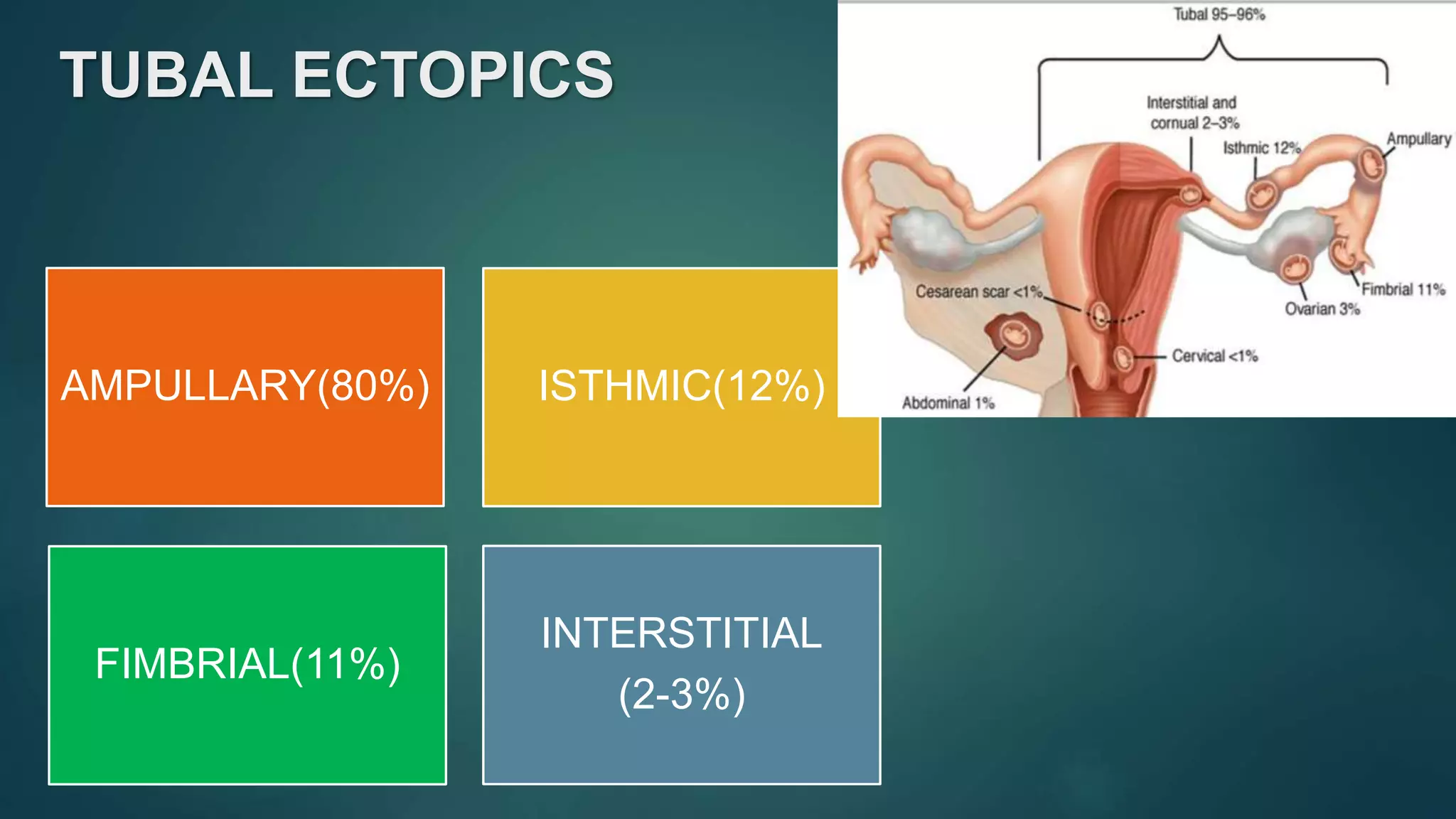
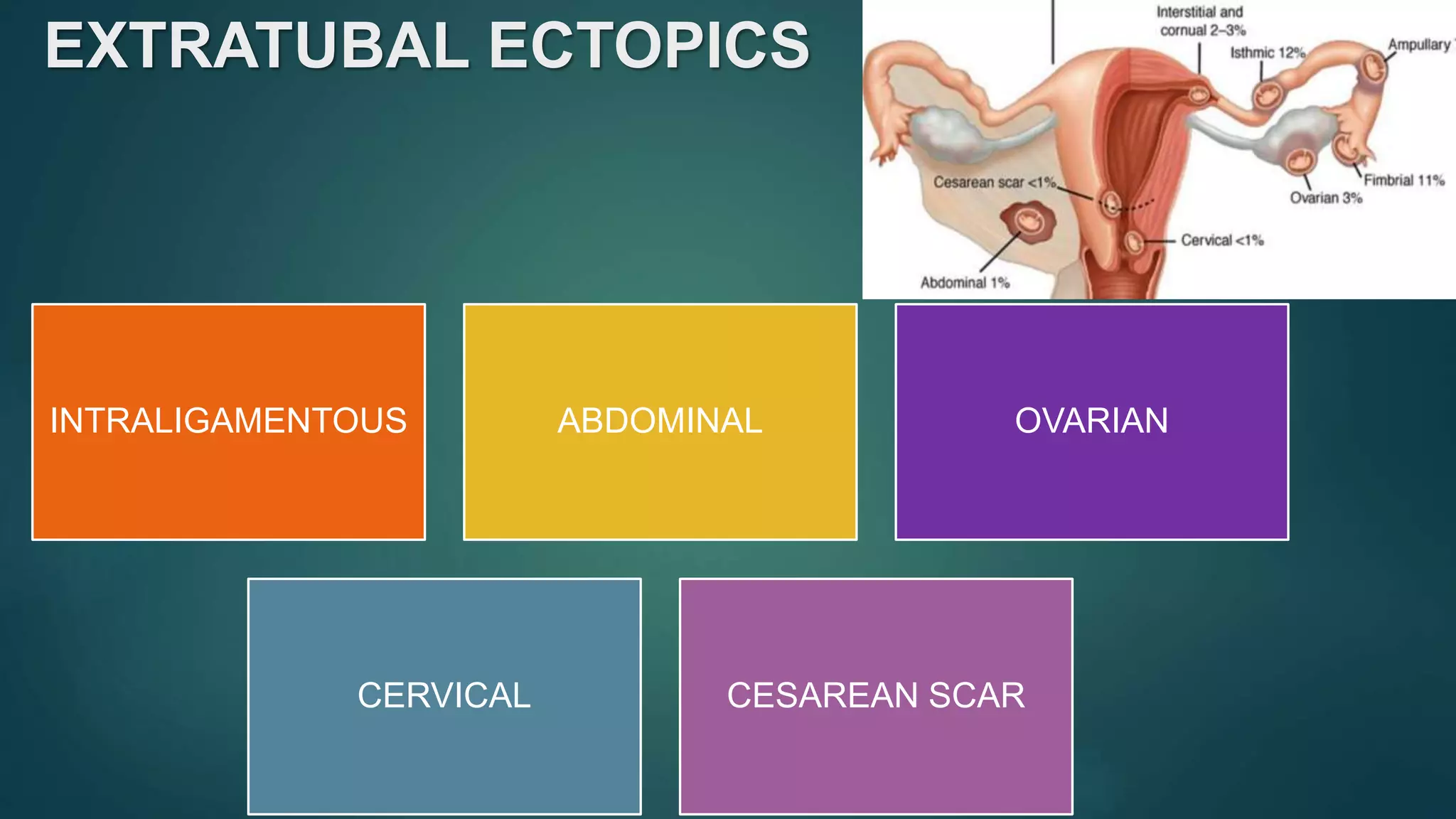
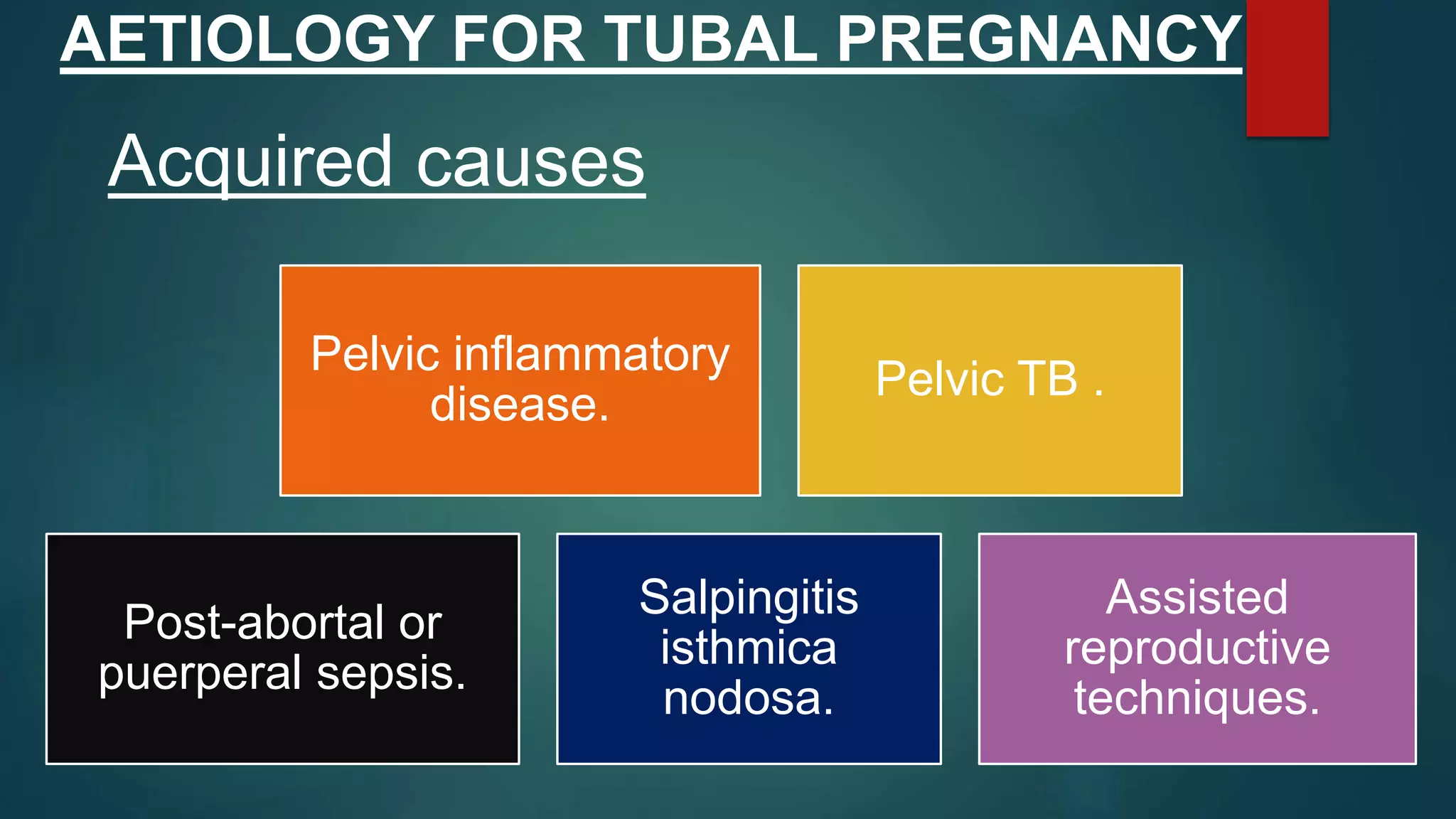
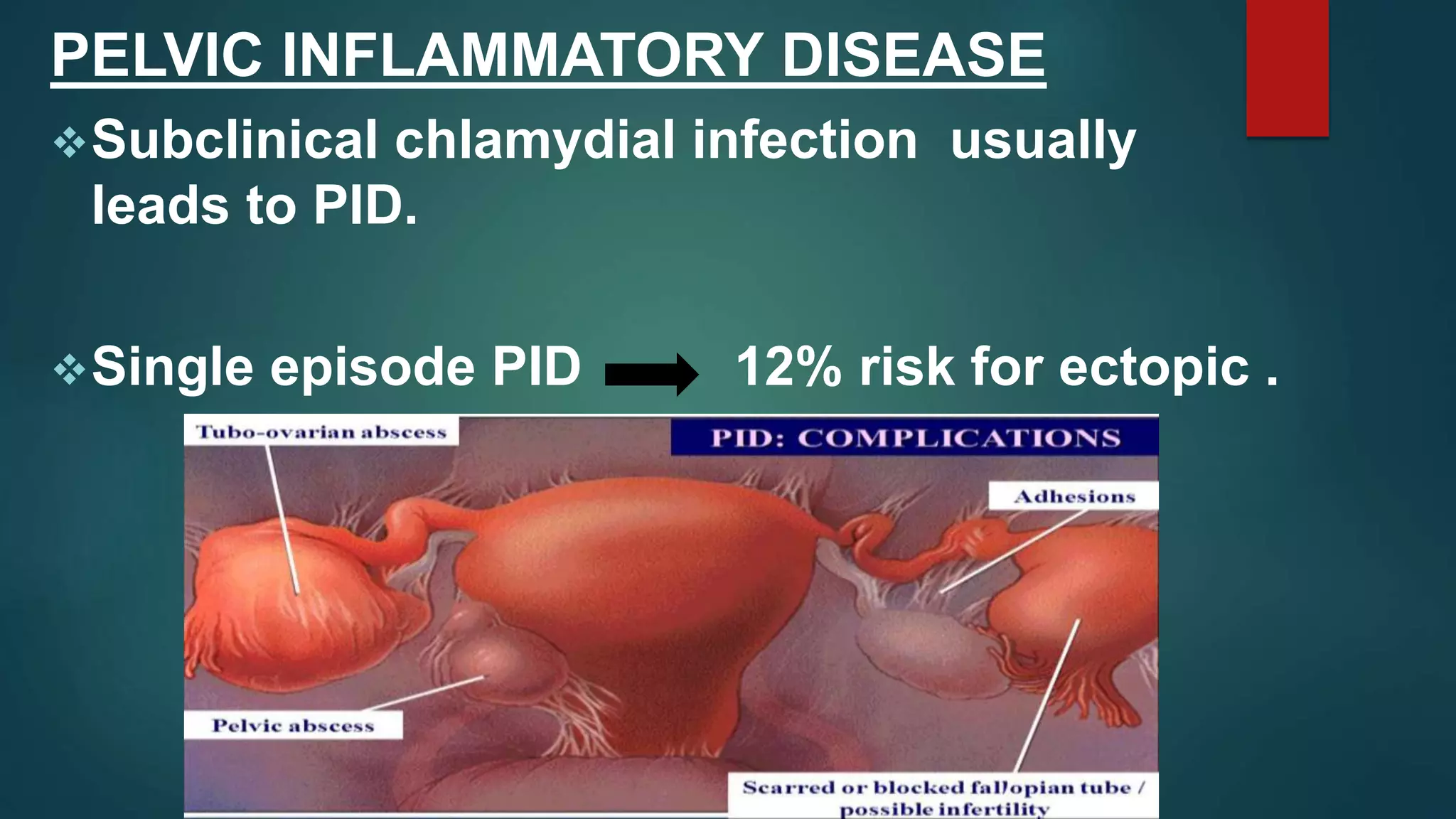
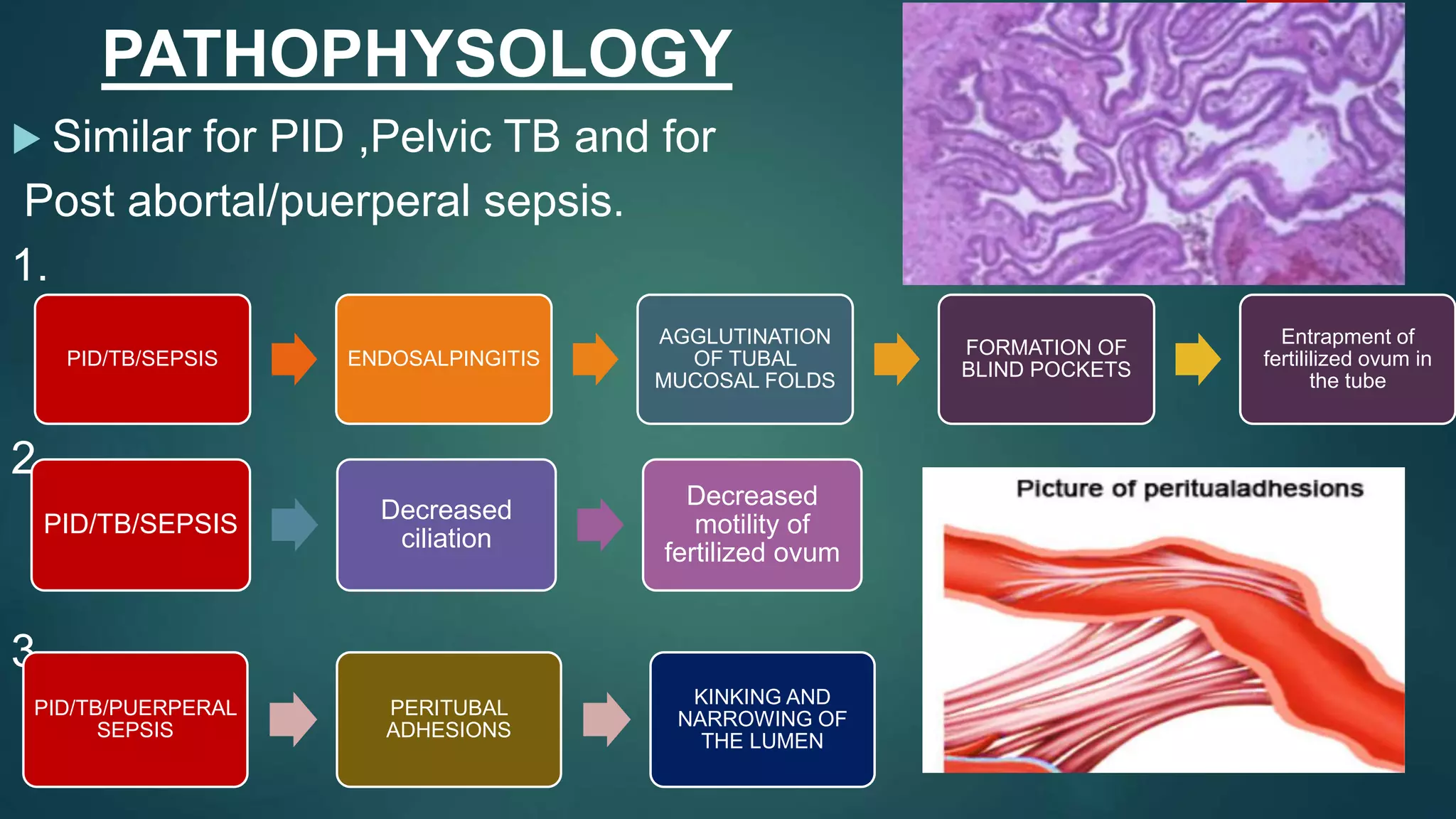
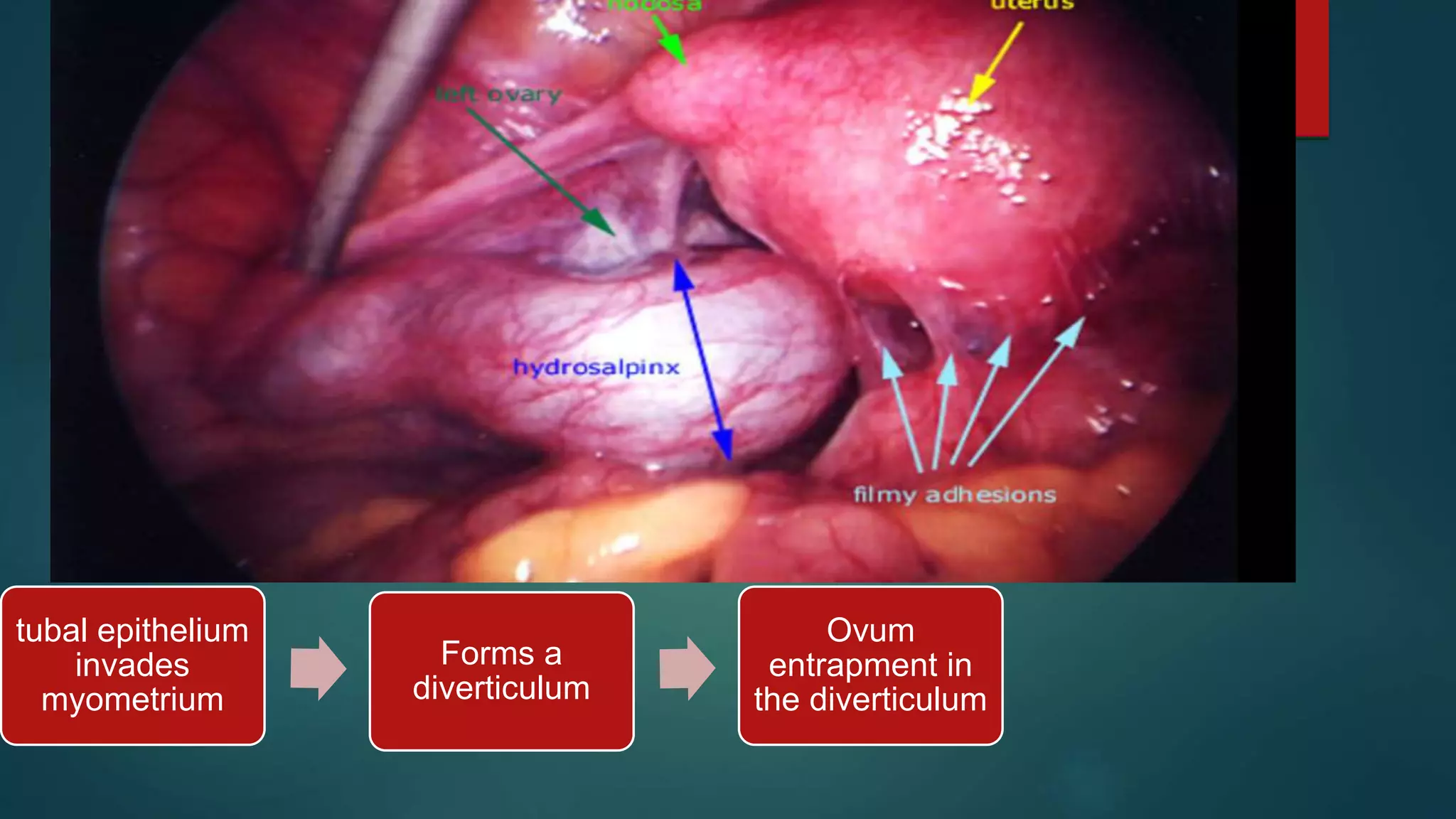
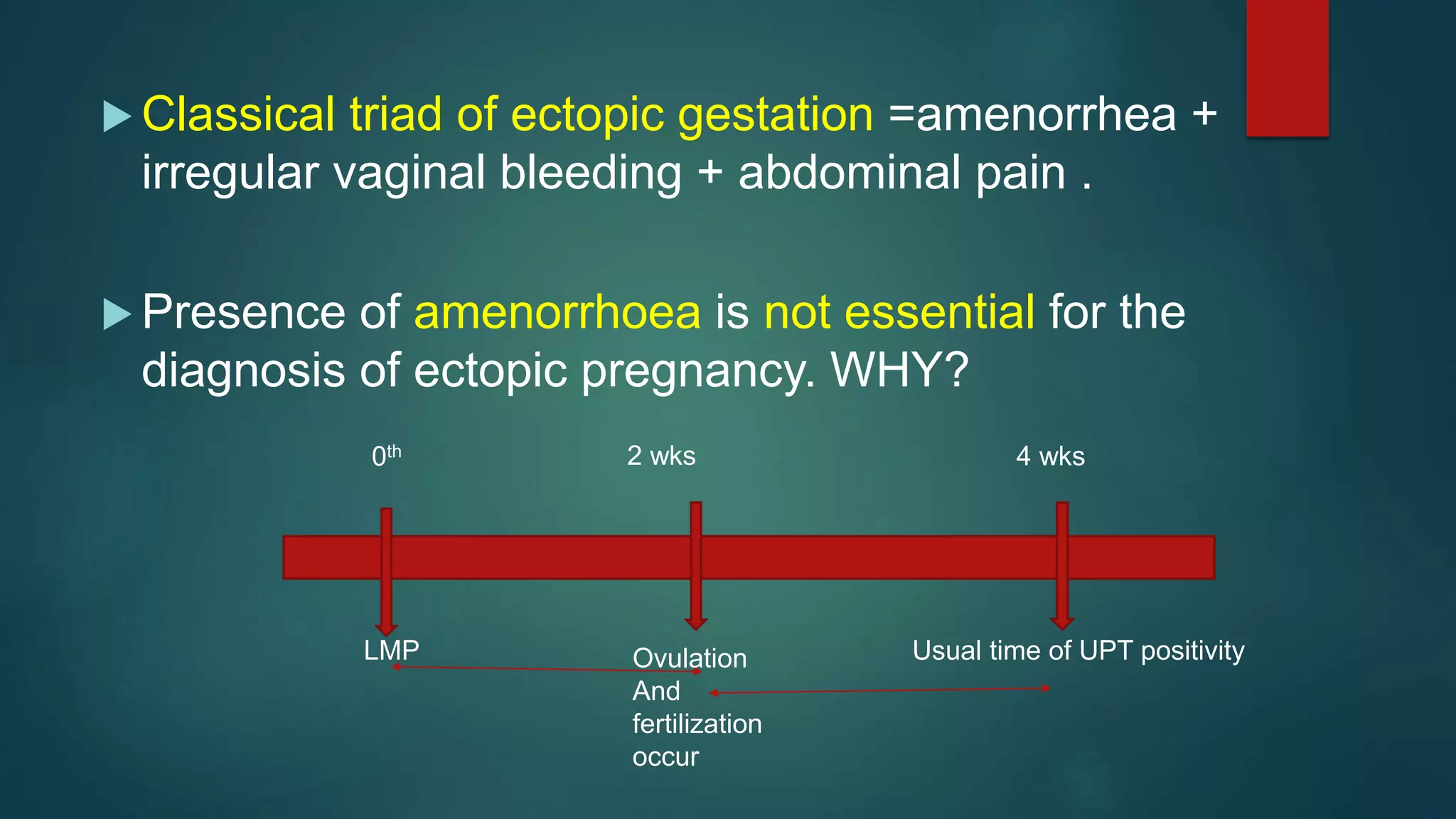
Ectopic pregnancies, which account for 1-2% of reported pregnancies, are on the rise due to factors such as increased STD prevalence and enhanced diagnostic methods. The majority of ectopic pregnancies occur in the fallopian tubes, and risk factors include pelvic inflammatory disease, assisted reproductive techniques, and previous surgeries. Symptoms can include amenorrhea, abdominal pain, and vaginal bleeding, with the classical triad being amenorrhea, irregular bleeding, and abdominal pain.