An ectopic pregnancy occurs when a fertilized egg implants and grows outside the uterus, most commonly in the fallopian tubes. Risk factors include pelvic inflammatory disease, previous ectopic pregnancy, infertility treatments, and IUD use. Symptoms include abdominal pain, vaginal bleeding, and a positive pregnancy test. Diagnosis is often made using transvaginal ultrasound and beta-hCG levels. Treatment depends on whether the ectopic pregnancy has ruptured but may include medication with methotrexate or laparoscopic or open surgery to remove the ectopic pregnancy. The incidence of ectopic pregnancy is rising but maternal mortality is falling due to earlier diagnosis and treatment.
Introduction
The termectopic comes from the greek “ ektopis”
meaning displacement.
ek-out of + topos- Place = out of place.
The first person to use “ectopic” was obstetrician
Robert Barnes (1817-1907) who applied it to an extra
uterine pregnancy: an ectopic pregnancy.
3.
DEFINITION
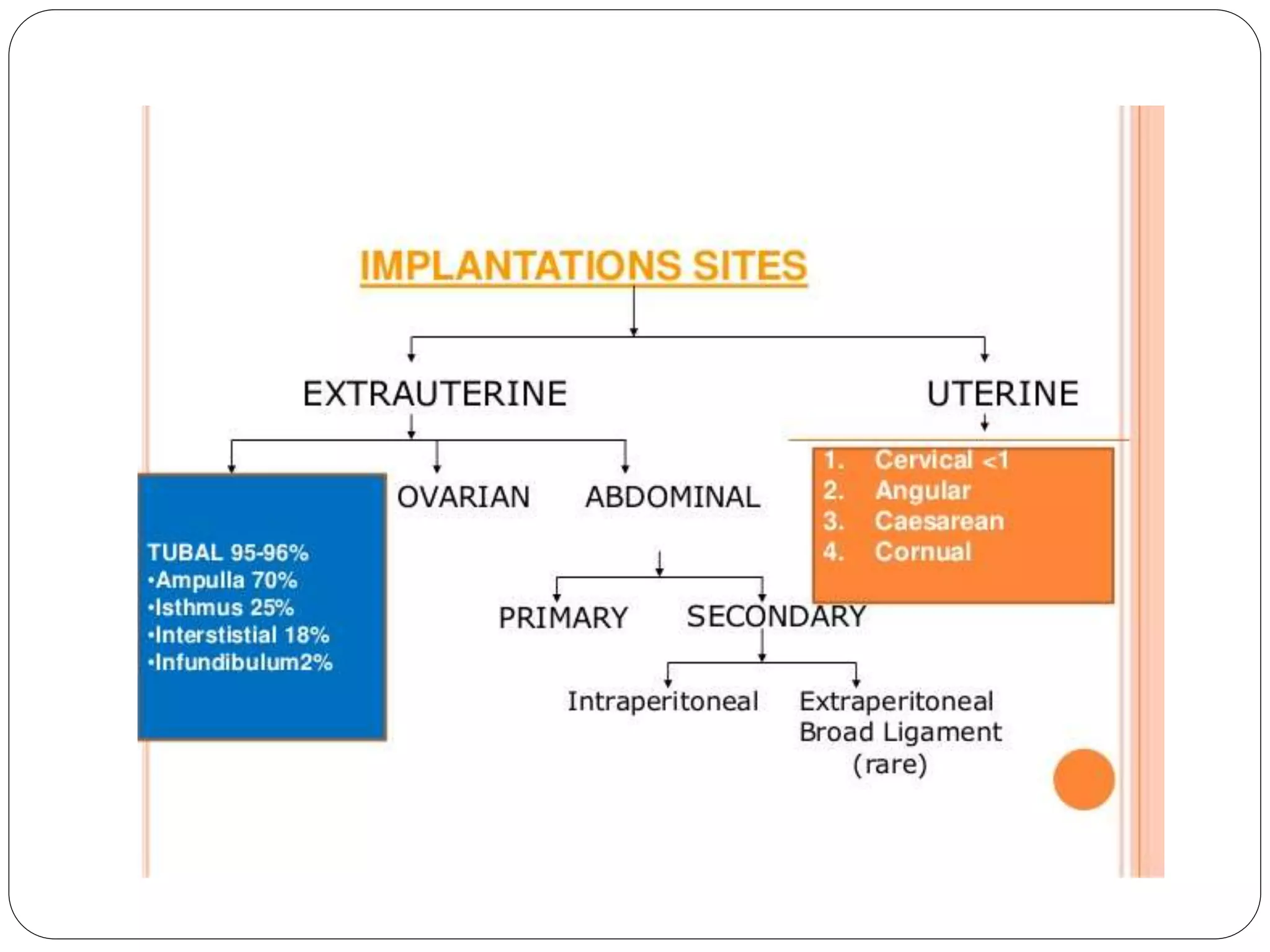
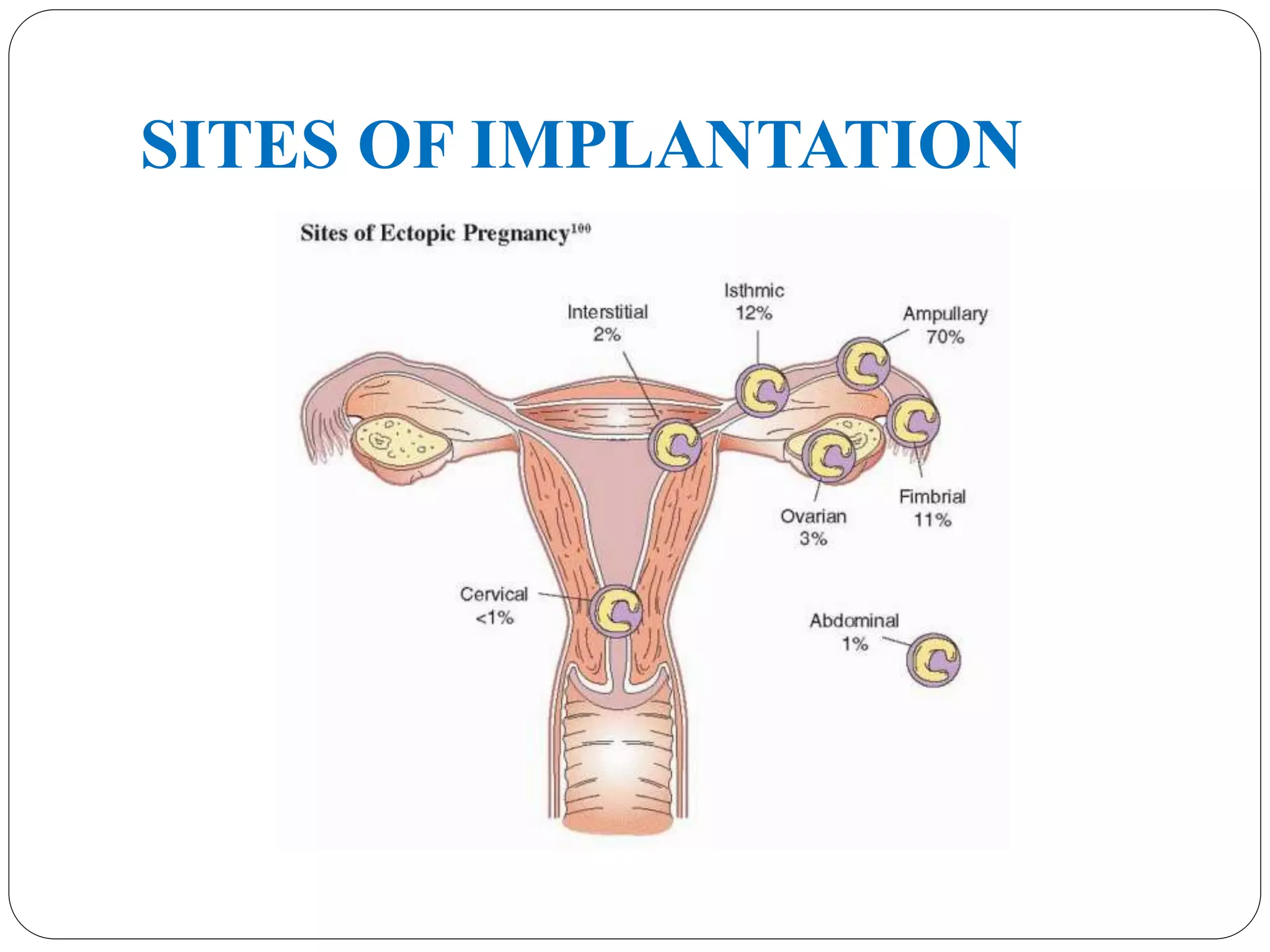
Any pregnancywhere the fertilized ovum gets
implanted & develops in a site other than normal
uterine cavity.
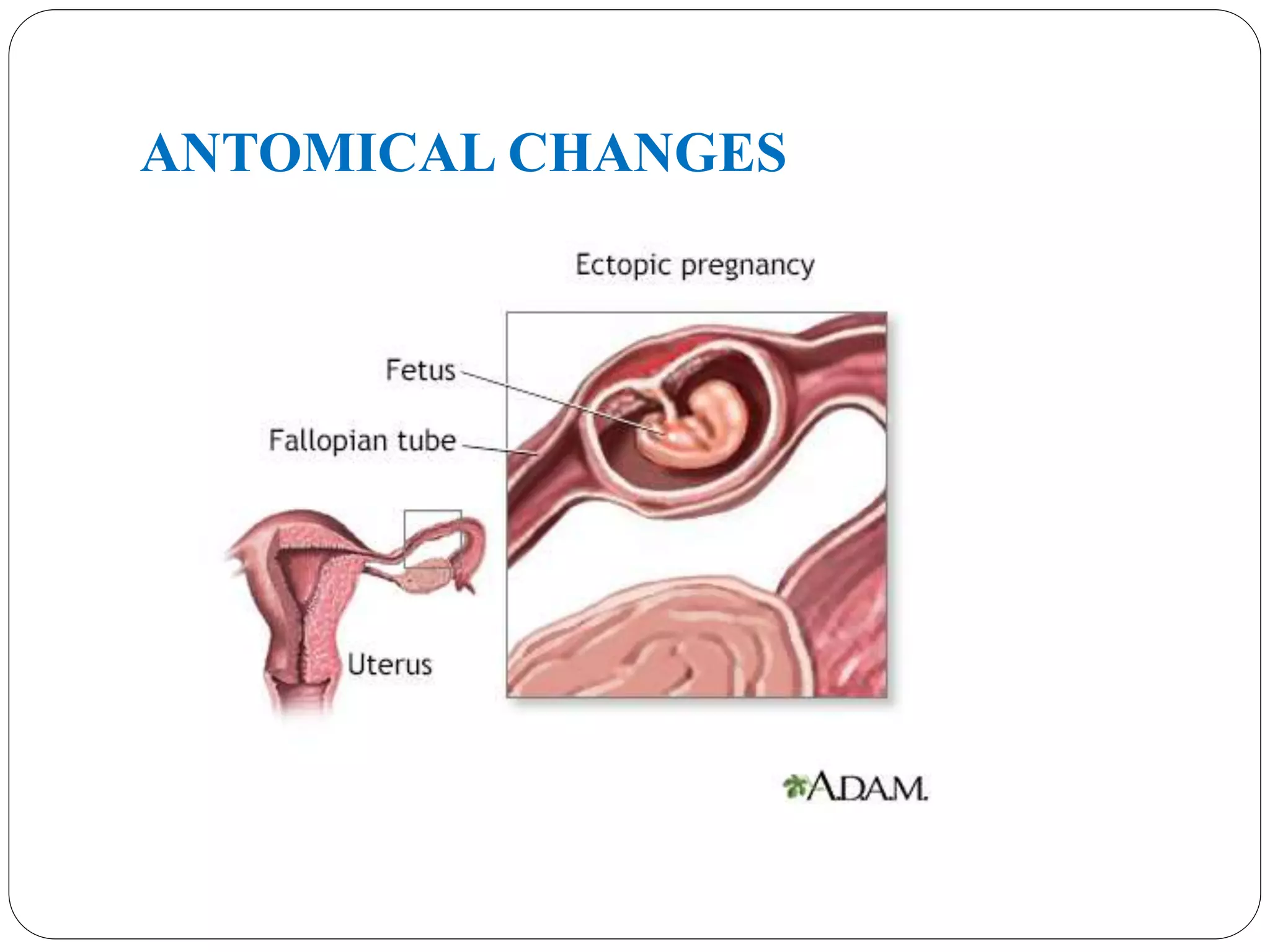
Ectopic pregnancy: fertilized embryo implanted
outside the uterine cavity.
ETIOLOGY
Any factorthat causes delayed transport of the
fertilized ovum through the tube.
Fallopian tube favors implantation in the tubal mucosa
itself thus giving rise to a tubal ectopic pregnancy.
These factors may be Congenital or Acquired.
ETIOLOGY
ACQUIRED
1. Infections
STIs& Pelvic Inflammatory disease (6-10 times)
Chlamydia trachomatis is most common
post abortal sepsis, puerperal sepsis & appendicitis
Genital TB is an important cause in India.
ETIOLOGY
3.Tubal suregry
Tubal reconstructivesurgery (4-5 times), tuboplasty,
salpingotomy.
4. Assisted Reproductive technique
Ovulation induction, IVF-ET and GIFT (4-7%) –
Risk of heterotopic pregnancy(1%)
5.Previous Ectopic Pregnancy - 7-15% chances of repeat
ectopic pregnancy
12.
Other Risk factors
Age 35-45 yrs
Previous induced abortion
Previous pelvic surgeries
Cigarette smoking
DES Exposure in Utero
Infertility
13.
Other Risk factors
Salpingitis Isthmica Nodosa
Genital Tuberculosis
Fundal Fibroid
Adenomyosis of tube
Transperitoneal migration of ovum
14.
MORBID ANATOMY
Implantation- intercolumnaror between mucosal folds
Decidual change minimal
Muscle hyperplasia & Hypertrophy min.
Intramuscular implantation
Pseudo capsule formation
Trophoblast invasion-erosion of blood vessel
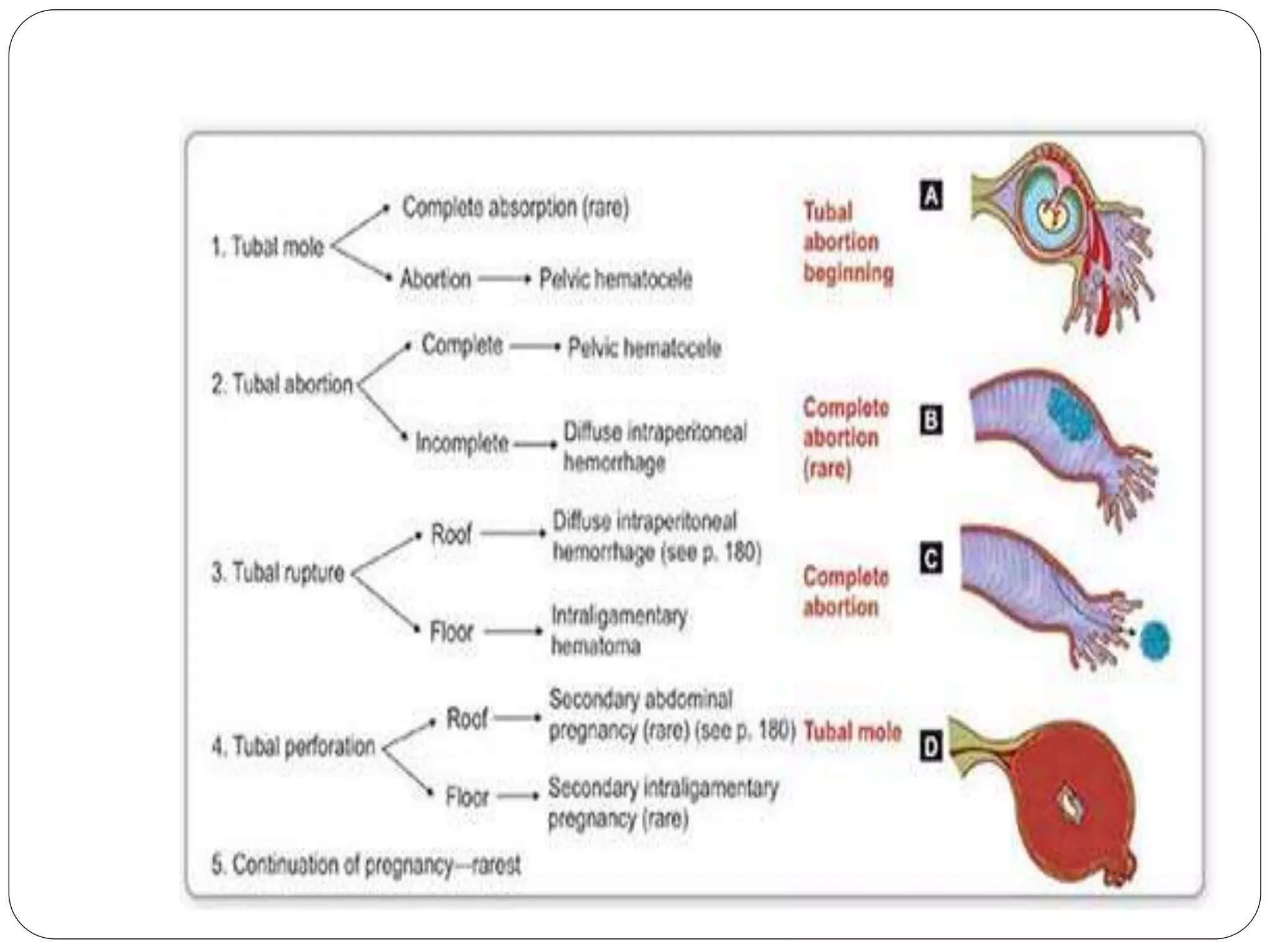
The pregnancy is unable to survive owing to its poor
blood supply, thus resulting in a tubal abortion and
resorption, (rare), Tubal Rupture
ACUTE ECTOPIC PREGNANCY
Classicaltriad is present in 50% of pt with rupture
ectopic.
PAIN:- most constant feature in 95% pt. Pain may be
sharp, stabbing or tearing in nature.
The pain referred to the shoulder due to diaphragmatic
irritation by blood is called Danforth’s sign
18.
ACUTE ECTOPIC PREGNANCY
AMENORRHOEA:- 60-80% of pt - there may be
delayed period or slight spotting at the time of
expected menses.
VAGINAL BLEEDING: - scanty dark brown, history
of passage of a fleshy mass vaginally.
Feeling of nausea, vomiting, fainting attack, syncope
attack(10%) due to reflex vasomotor disturbance.
Dysuria, frequency or retention of urine
Rectal tenesmus
19.
EXAMINATION
O/E:- patient isrestless in agony, looks blanched, pale,
sweating with cold clammy skin. Features of shock,
tachycardia, hypotension
P/A:- abdomen tense, tender mostly in lower
abdomen, shifting dullness, rigidity may be present.
Cullen’s sign: periumbilical bluish discoloration due to
intraperitoneal bleeding.
21.
Cont…
P/S:- minimalbleeding may be present
P/V:- uterus may be bulky, deviated to opposite side,
fornix is tender, excitation pain on movement of
cervix. POD may be full, uterus floats as if in water.
22.
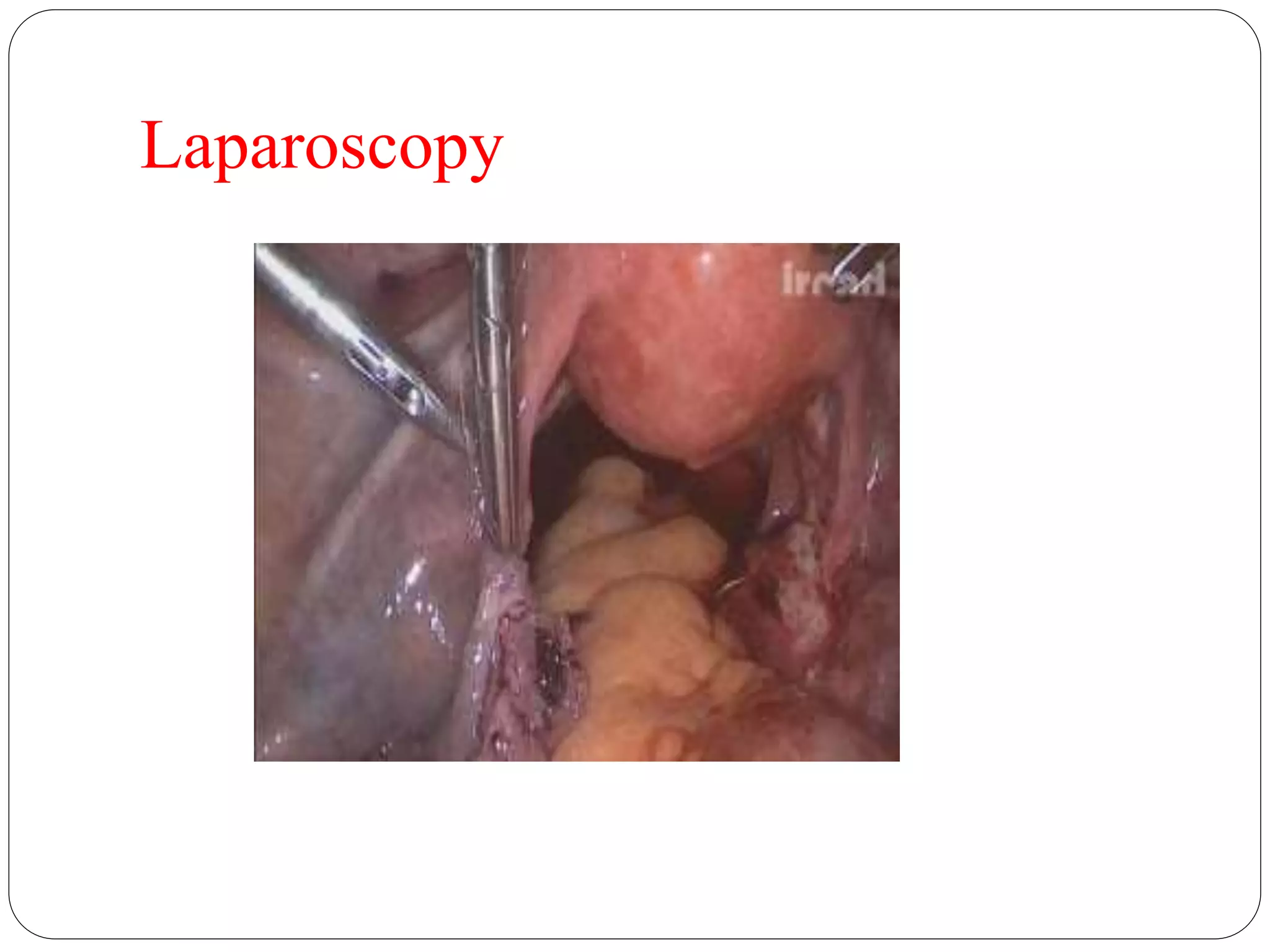
UNRUPTURED ECTOPIC
Diagnosed accidentallyin Laparoscopy or Laparotomy
C/F – delayed period, spotting with discomfort in
lower abdomen.
P/A - tenderness in lower abdomen
P/V - should be done gently
uterus is normal size, firm
small tender mass may be felt in the fornix
Investigations- TVS, radioimmunoassay of β-HCG and
Laparoscopy
24.
DIAGNOSIS
Patient withacute ectopic can be diagnosed clinically.
Blood should be drawn for Hb%, CBC, blood
grouping and cross matching, Serology and
Coagulation profile.ESR high, leucocytosis up to
30,000/ml.
Urine pregnancy test:- positive in 95% cases.
ELISA is sensitive to 10-20 mlU/ml of β hCG
25.
DIAGNOSIS
Transvaginal Sonography (TVS):
Is more sensitive
It detect intrauterine gestational sac at 4-5wks
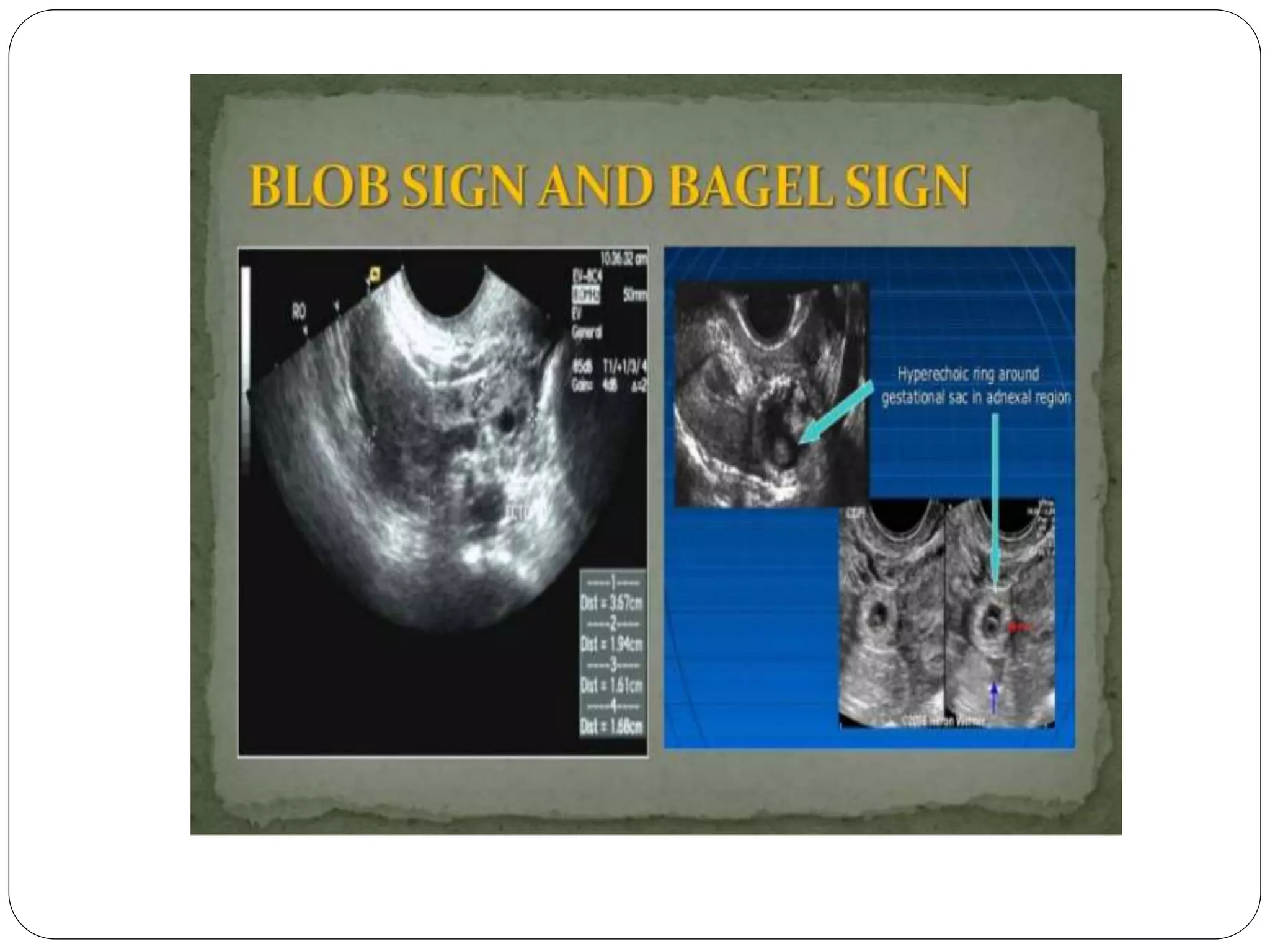
‘Bagel’ sign – Hyperechoic ring around gestational sac
in adnexal region
‘Blob’ sign – Seen as small inconglomerate mass next
to ovary with no evidence of sac or embryo.
color doppler by showing increased vascularity (ring-
of-fire pattern)
27.
DIAGNOSIS
Serum Progesterone –
level >25 ngm/ml is suggestive of normal intrauterine
pregnancy.
level <15 ngm/ml is suggestive of Extrauterine
pregnancy.
<5 ngm/ml is suggestive nonviable pregnancy.
28.
DIAGNOSIS
Diagnostic Laparoscopy(Gold standard)– Can be done
only when patient is haemodynamically stable.
It confirms the diagnosis and removal of ectopic mass
can be done at the same time.
MANAGEMENT OF ECTOPIC
PRINCIPLE: Resuscitation and Laparotomy/
Laparoscopy
ANTI SHOCK TREATEMENT: - IV line made patent,
crystalloid is started - Blood sample for Hb, blood
grouping & cross matching, BT, CT - Folley’s
catheterization done - Colloids for volume replacement
33.
MANAGEMENT OF ECTOPIC
LAPAROTOMY:
-Principle is ‘Quick in and Quick out’
-Rapid exploration of abdominal cavity is done
- Salpingectomy is the definitive surgery (sent for HP
study)
- Blood transfusion to be given
34.
MANAGEMENT OF ECTOPIC
Laparoscopy
Preferred method if haemodynamically stable
Tubal Patency no significant difference
Shorter operative time
Salpingostomy
Less than 2cm size
10-15mm incision
35.
MANAGEMENT OF UNRUPTURED
ECTOPICPREGNANCY
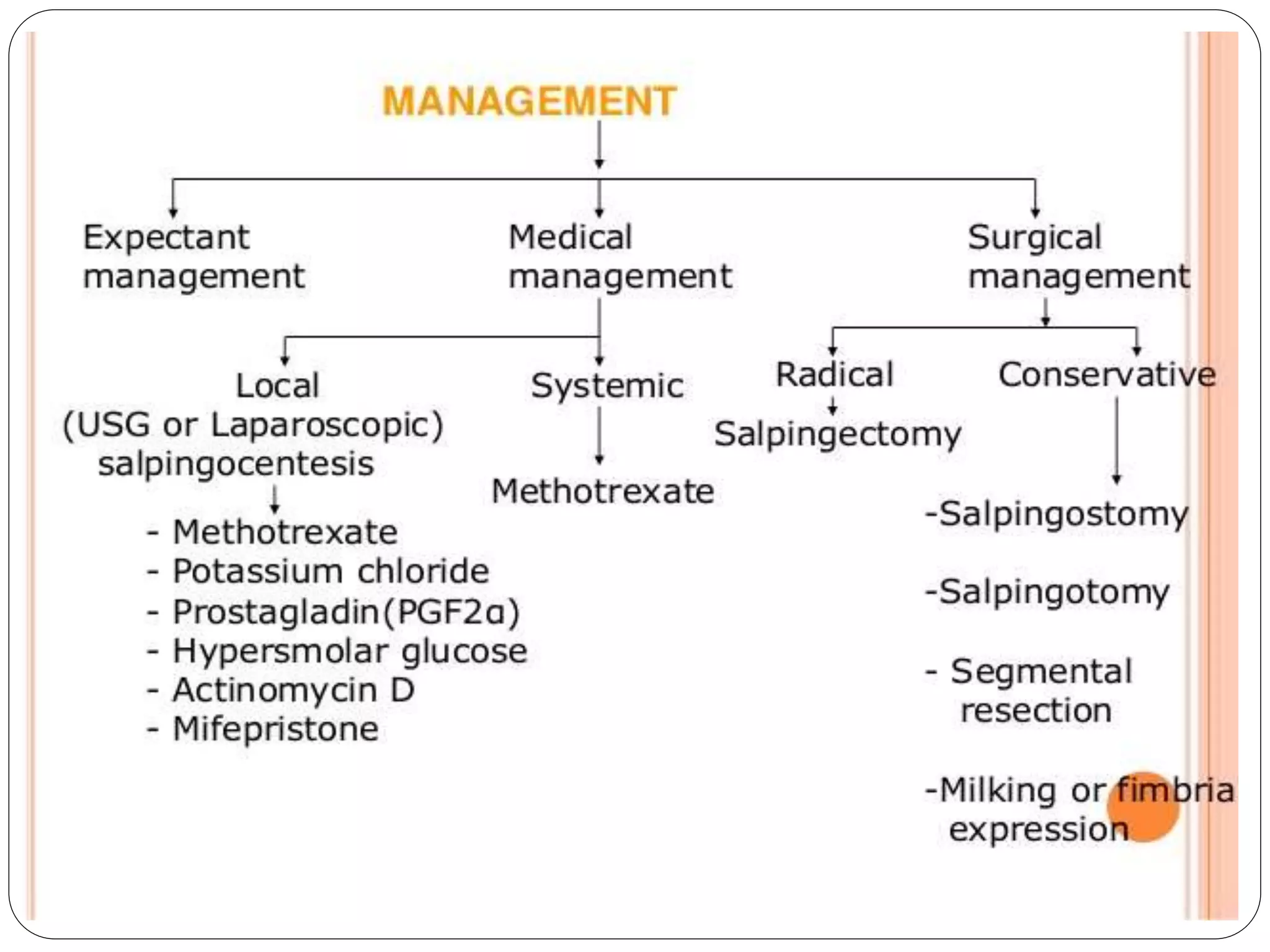
MEDICAL MANAGEMENT:
METHOTREXATE (MTX) single dose 50 mg per m2
body surface (1mg per kg body weight) IM.
Conservative Surgery : Can be done Laparoscopically or
by microsurgical laparotomy
36.
VARIOUS CONSERVATIVE
SURGERIES
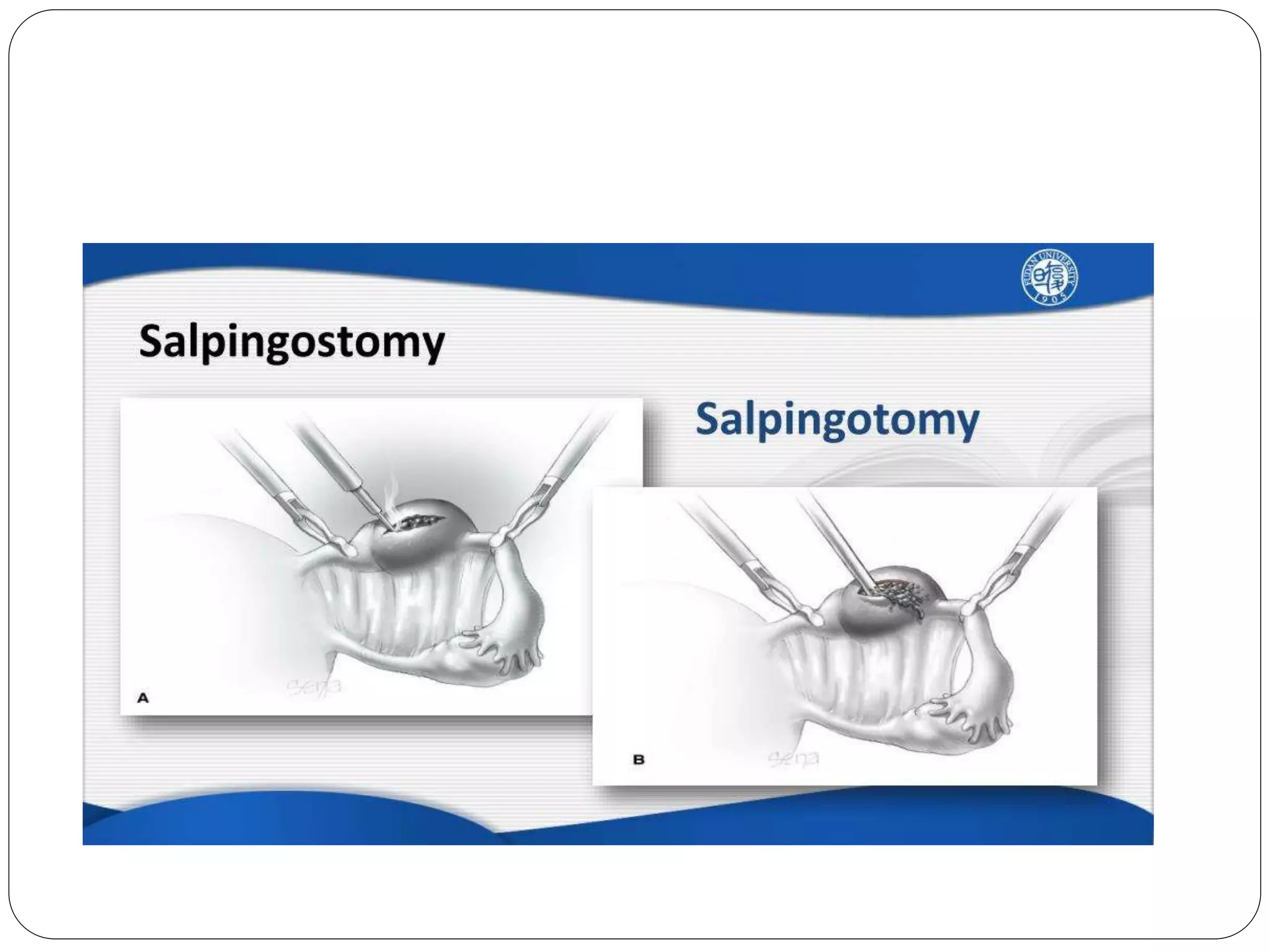
1.Linear Salpingostomy:- Indicated in unruptured
ectopic. Linear incision given on antimesentric border
over the site and product removed by fingers, scalpel
handle or gentle suction and irrigation.
Incision line kept open (heals by secondary intention)
2. Linear Salpingotomy : - Incision line is closed in two
layers with 7-0 interrupted vicryl sutures.
38.
VARIOUS CONSERVATIVE
SURGERIES
3. SegmentalResection & Anastomosis: - Indicated in
unruptured isthmic pregnancy
End to end anastomosis is done immediately or at later
date
4. Milking or fimbrial Expression: - This is ideal in distal
ampullary or infundibular pregnancy.
It has got increased risk of persistent ectopic pregnancy.
39.
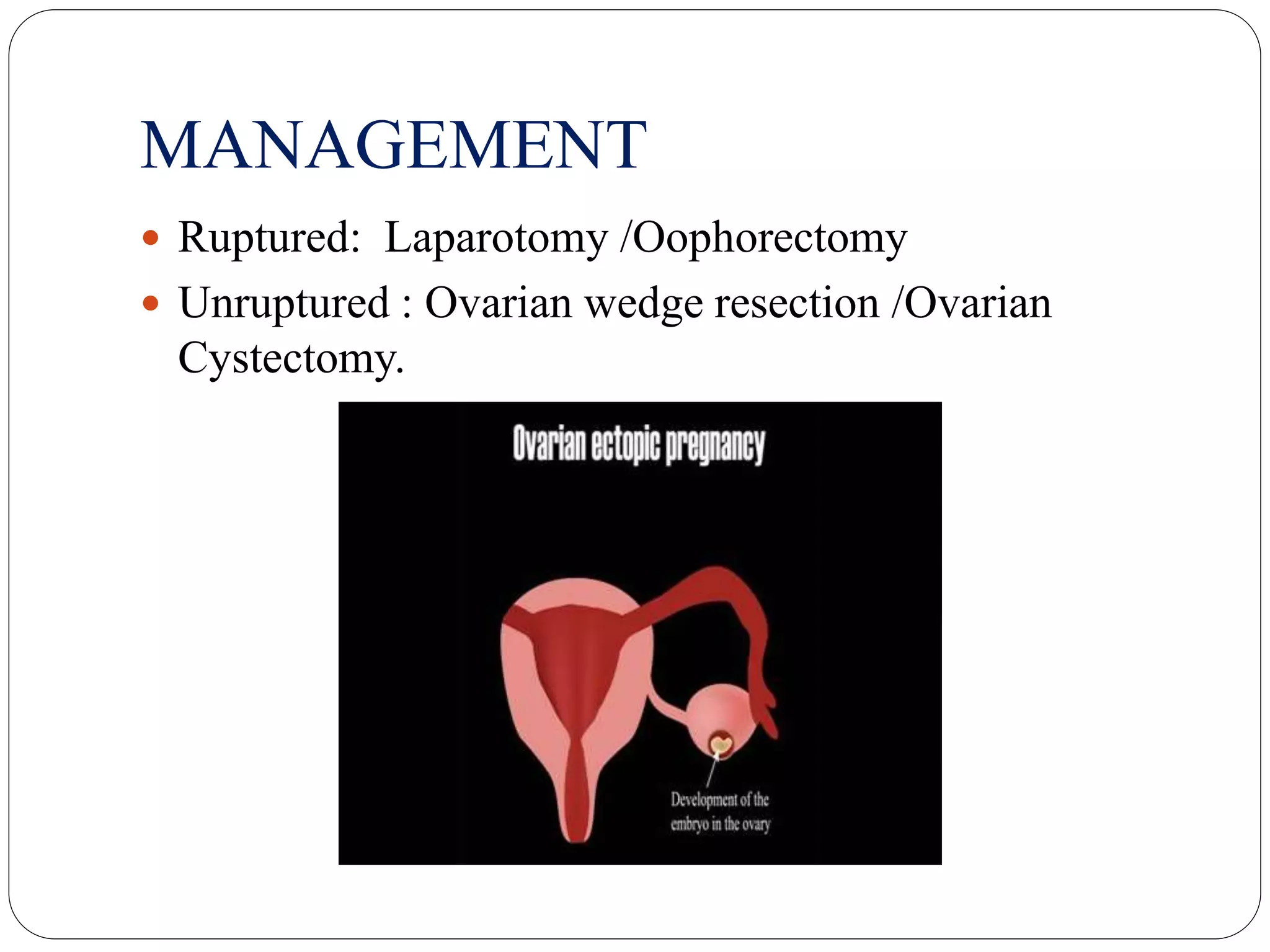
OVARIAN ECTOPIC PREGNANCY
Incidence: 1:40,000 Risk factor
Cause: IUCD - Endometriosis on surface of ovary
C/F are same as tubal pregnancy, ruptures within 2-3 wks
Diagnosis: On Laparotomy
Spiegelberg’s Criteria
1. tube in affected side must be intact and separate from sac
2. Sac occupies the position of the ovary
3. Connected to uterus by ovarian ligament
4. Ovarian tissue found on its wall on HP study
ABDOMINAL PREGNANCY
Incidence:Rarest
H/O : - Irregular bleeding, spotting - Nausea, vomiting,
flatulence, constipation, diarrhoea, abdominal pain. -
Fetal movement may be painful and high in the
abdomen
O/E : - Abnormal fetal position, easy in palpating fetal
parts. - uterus palpated separate from sac - no uterine
contraction after oxytocin infusion
42.
Abdominal pregnancy
Diagnosis:Confirmed by USG, CT scan, MRI,
Radiography
Studiford’s criteria 1. Both tubes and ovaries normal 2.
Absence of Uteroperitonal fistula 3. Pregnancy related
to Peritoneal surface & young enough to rule out
possibility of secondary implantation
43.
Management
Urgent Laparatomy irrespectiveof period of gestation
Ideal to remove entire sac fetus, placenta, membrane
Placenta may be left if attached to vital organs, get
absorbed by aseptic autolysis
44.
CERVICAL PREGNANCY
Implantationoccurs in cervical canal at or below
internal Os.
Incidence: 1 in 18,000
RISK FACTORS : - Previous induced abortion
- Previous caesarean delivery
- Asherman’s syndrome
- IVF
- DES exposure
- Leiomyoma
45.
CERVICAL PREGNANCY
CLINICAL CRITERIA:Paulman & McEllin
1. Uterine bleeding, no cramping, following
amenorrhoea
2. Cervix distended,thin walled,soft consistency
3. Enlarged uterine fundus may be palpated.
4. Internal Os is closed
5. External Os is partially opened
46.
MANAGEMENT
Hysterectomy
Cerclage :Mc Donald’sWharton ≈ Shirodkar’s –
Transvaginal ligation of Cx branch of uterine artery
Angiographic uterine A embolisation
Intracervical vasopressin inj
Foley’s catheter as tamponade
Medical Recently proposed Single or Combination OR
Adjunct to surgery - Methotrexate - Actinomycin
47.
HETEROTYPIC PREGNANCY
Co-existing intrauterineand extra uterine Pregnancies
Incidence: 1 : 30,000
With ART – 1:7000 –
With ovulation induction – 1:900
M/M : Depends on the site. Ectopic site may be removed with
continuation of IU pregnancy
48.
conclusion
Incidence ofectopic pregnancy is rising while maternal
mortality from it is falling.
Ectopic pregnancy can be diagnosed early (before it
ruptures) with recent advances in Immunoassay to detect β-
hCG , high resolution USG, and diagnostic Laparoscopy.
Laparotomy should be done when in doubt
The choice today is Laparoscopic treatment of un-ruptured
ectopic pregnancy.
Careful monitoring and proper counselling of patients is
mandatory