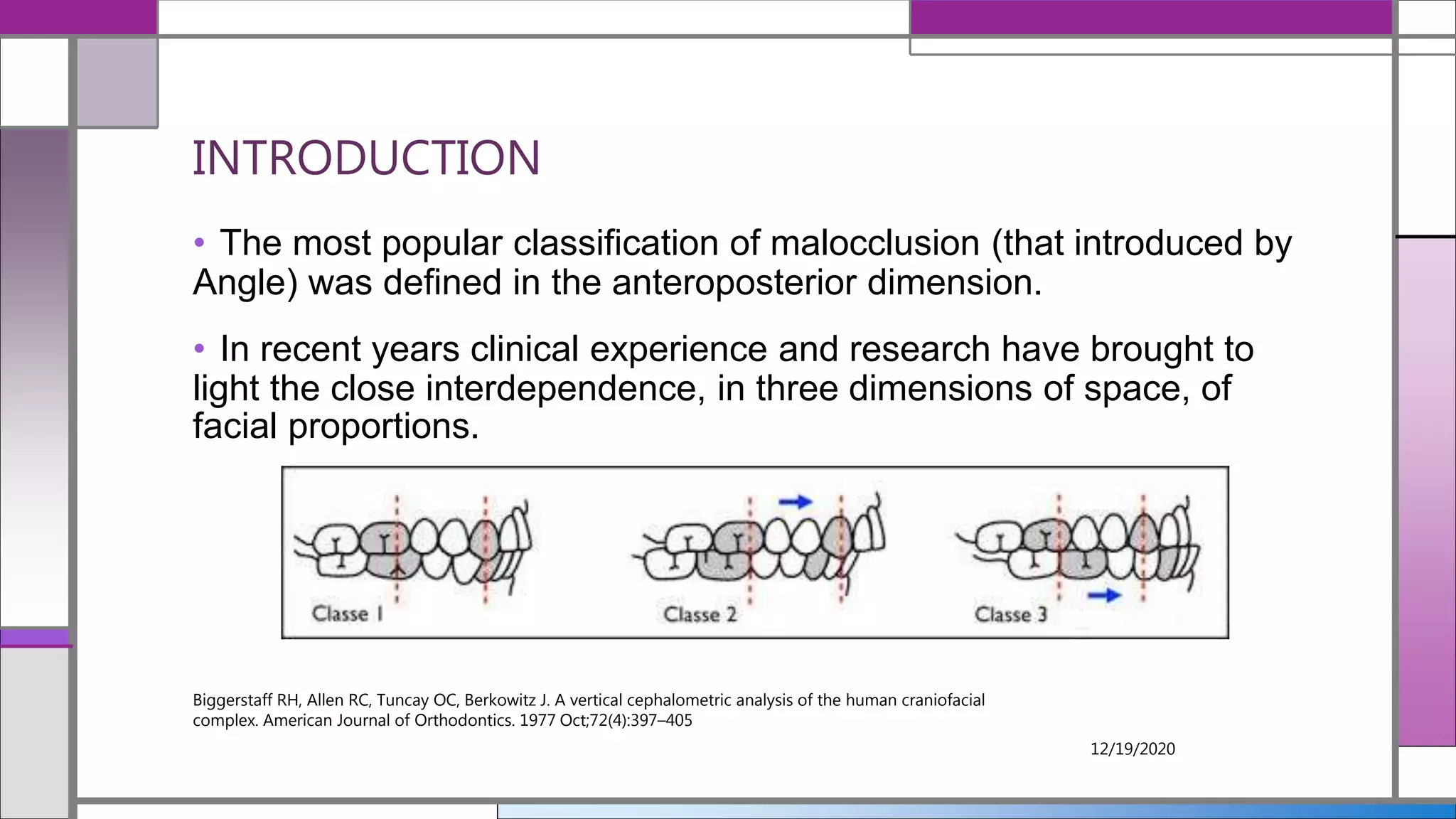
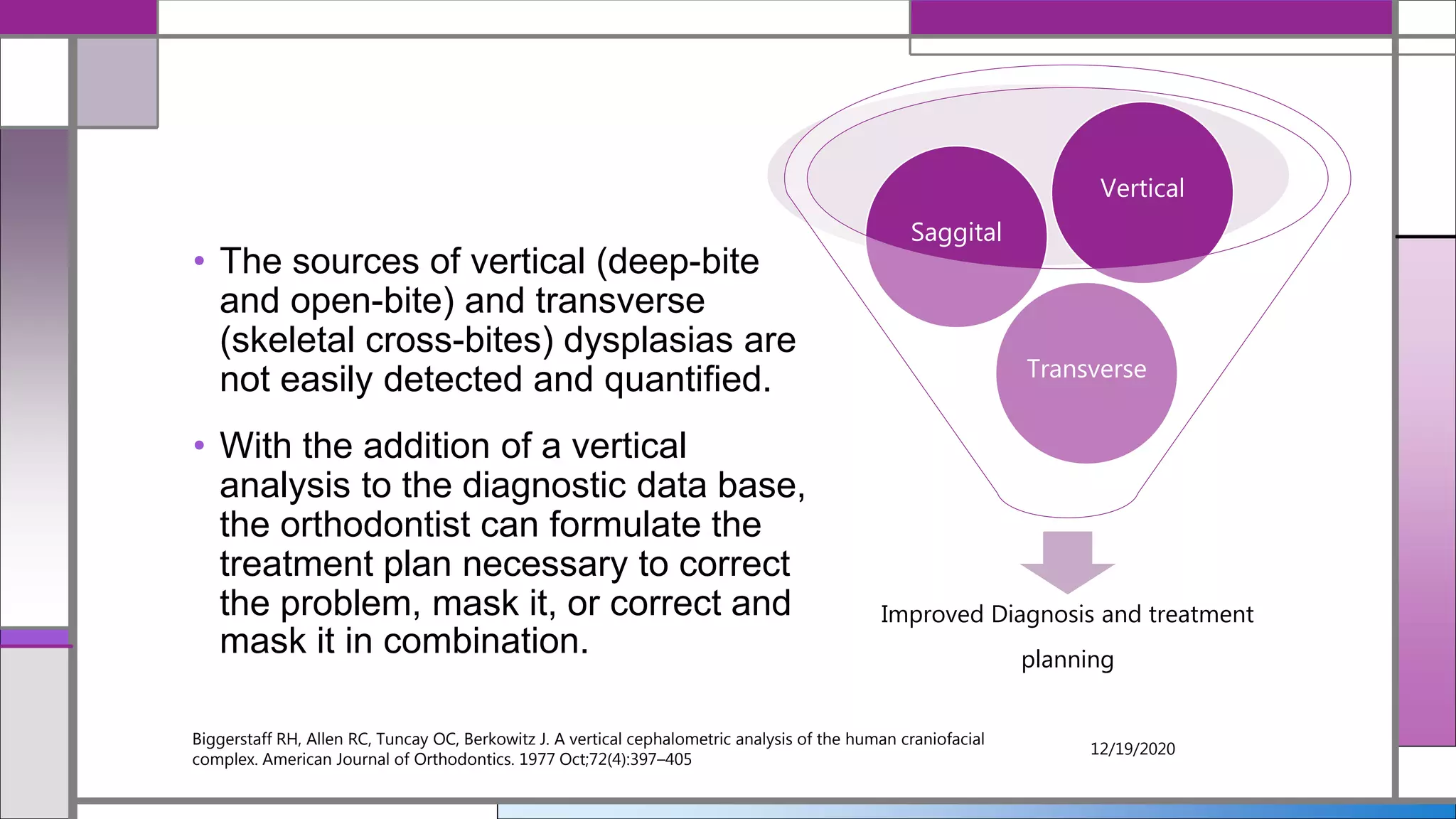
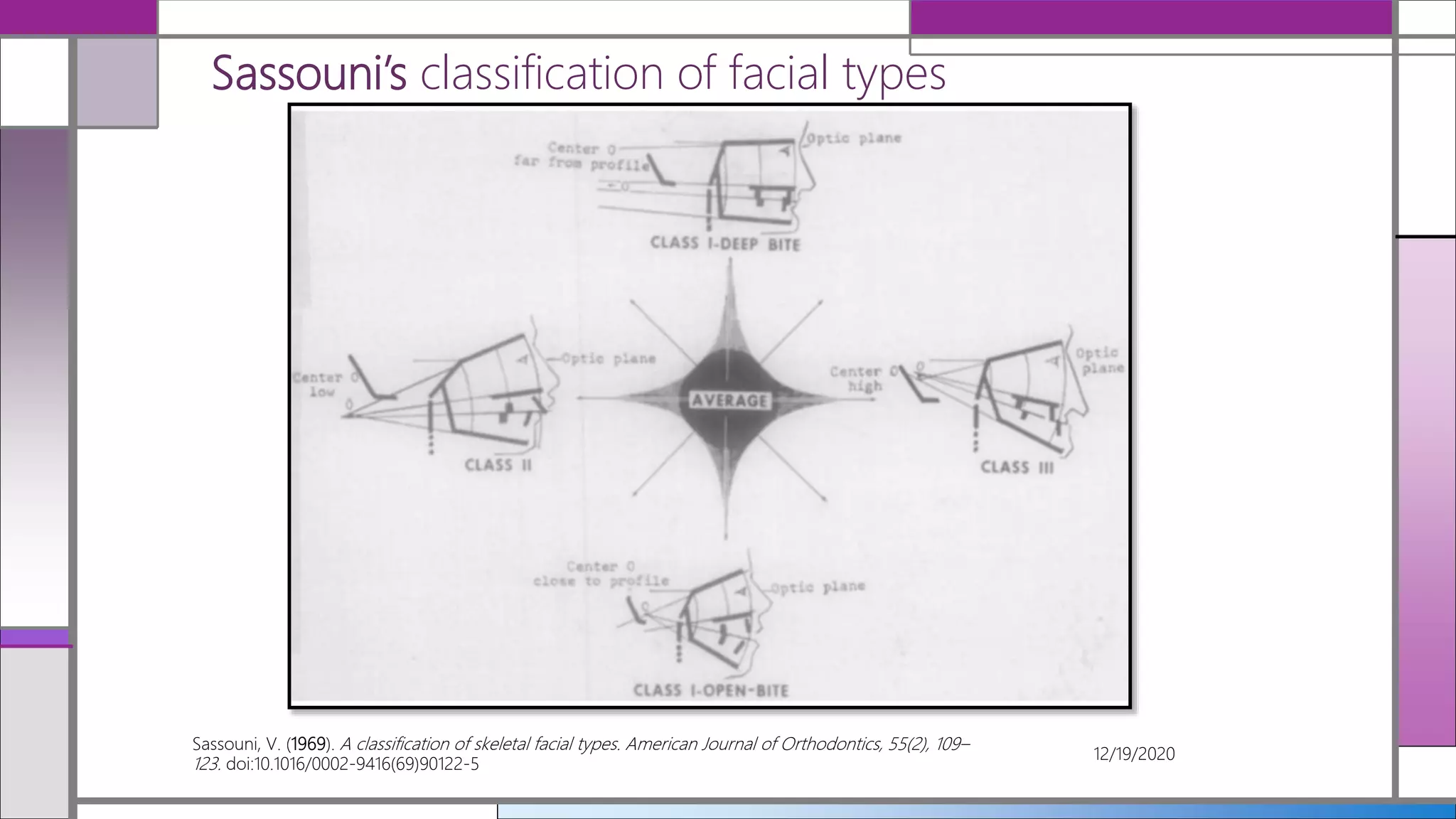
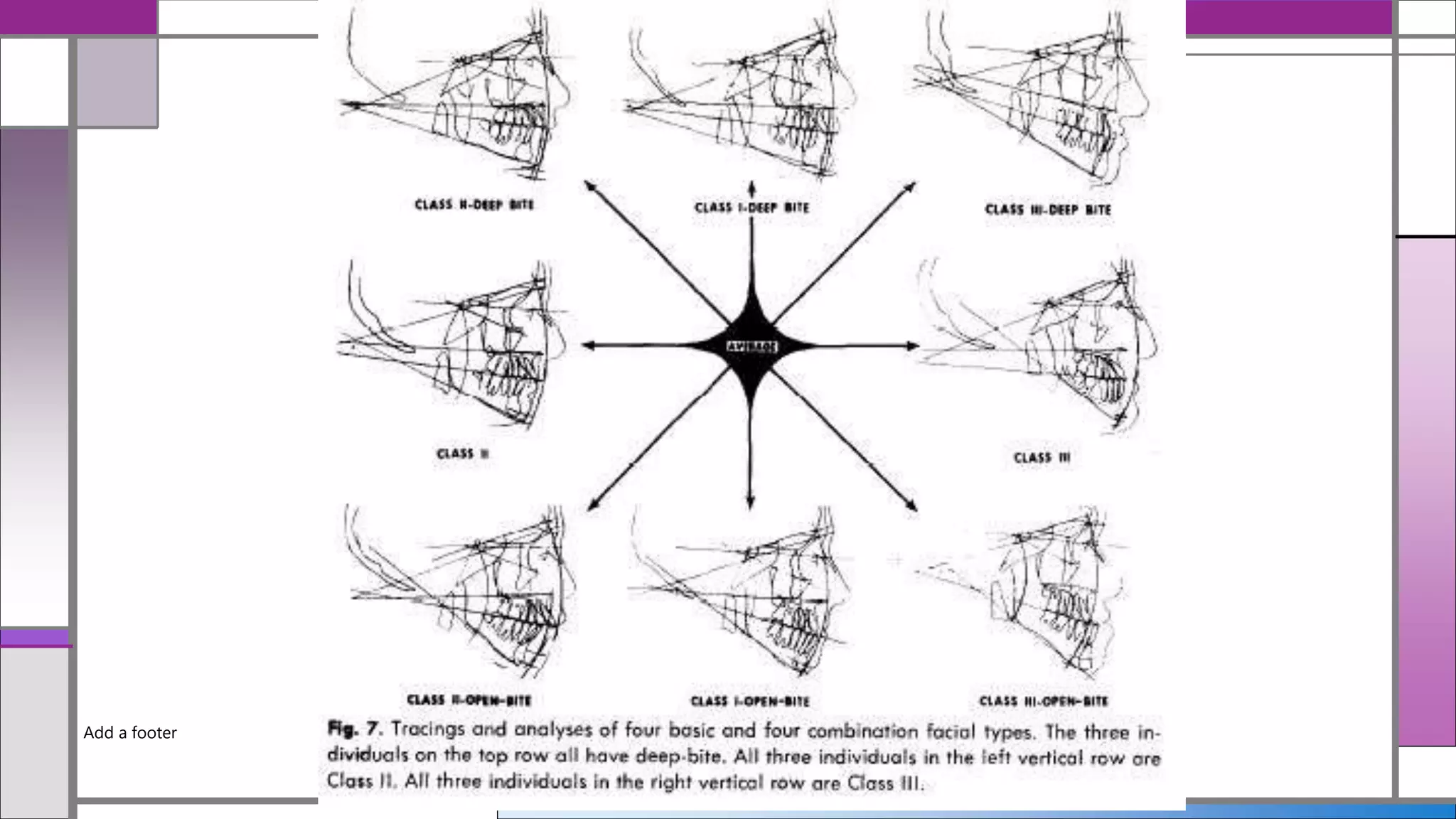
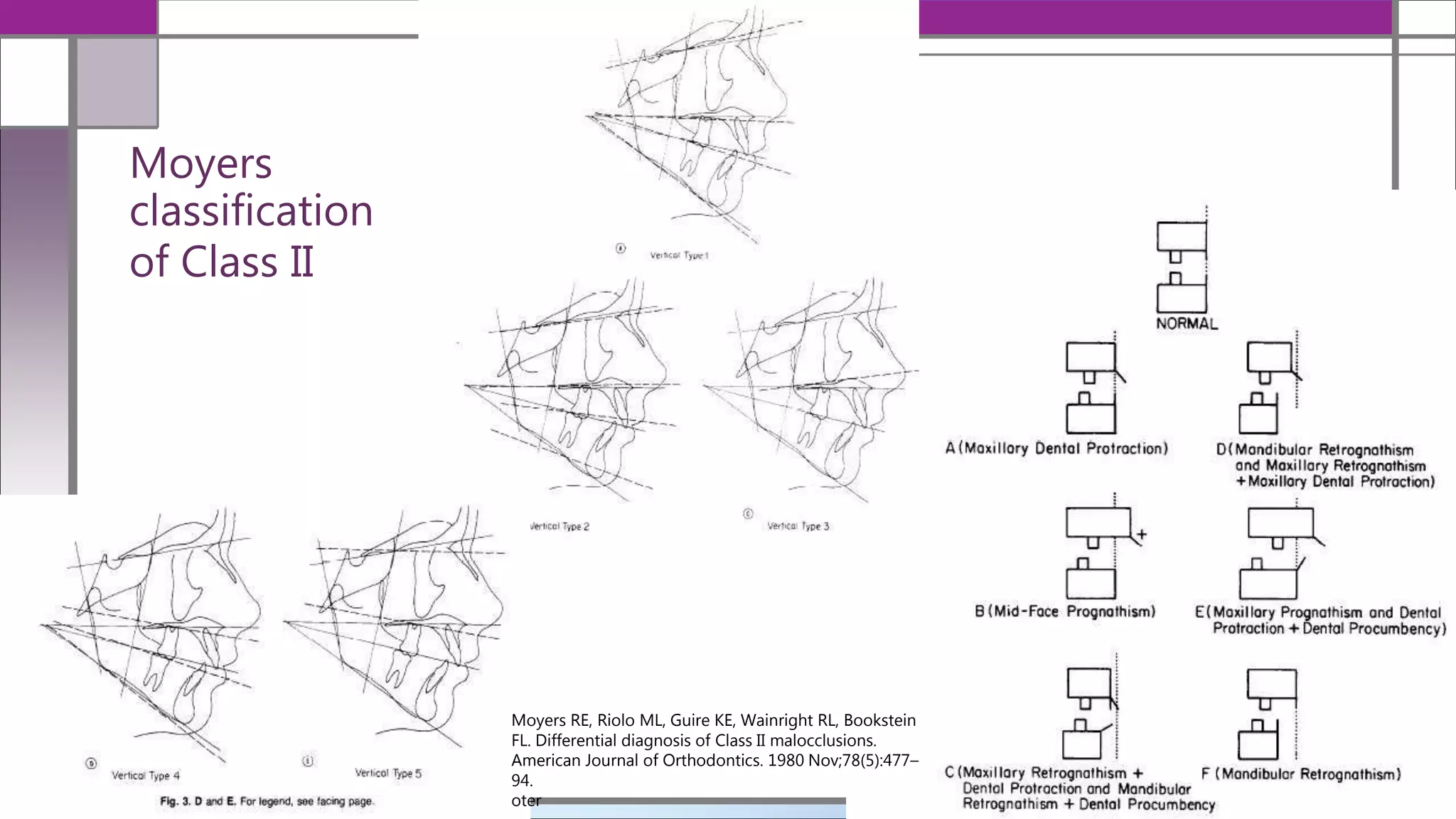
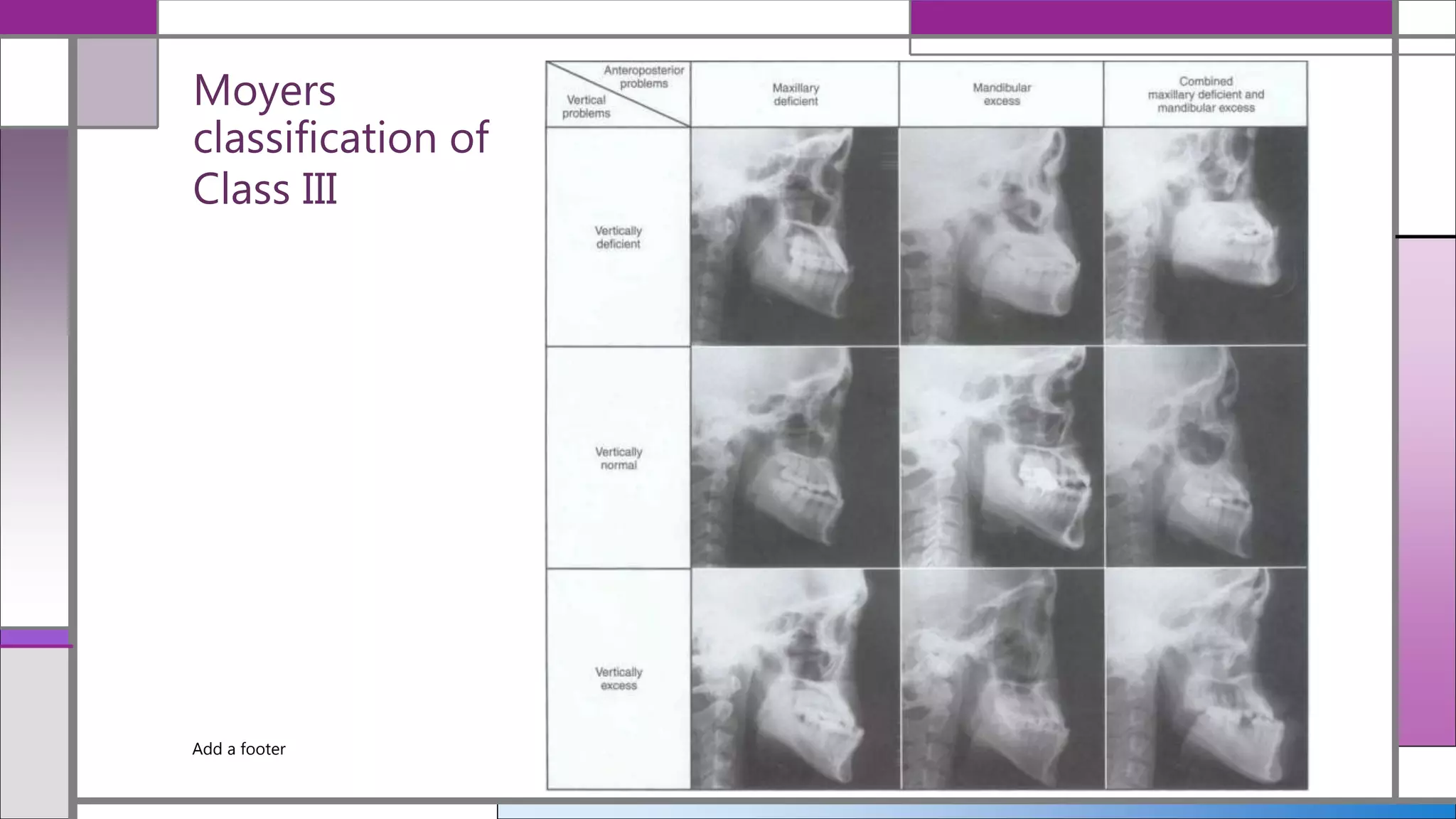
The document provides a comprehensive cephalometric analysis of vertical parameters, discussing various classifications of facial types and malocclusion, as well as methods to assess vertical maxillary excess. It outlines key analyses including Sassouni’s, Moyer’s, and Di Paolo's quadrilateral analysis, while emphasizing the importance of combining morphological knowledge with functional and aesthetic considerations for effective orthodontic treatment planning. The conclusion highlights the necessity for integrated approaches in cephalometric evaluations to achieve meaningful clinical outcomes.