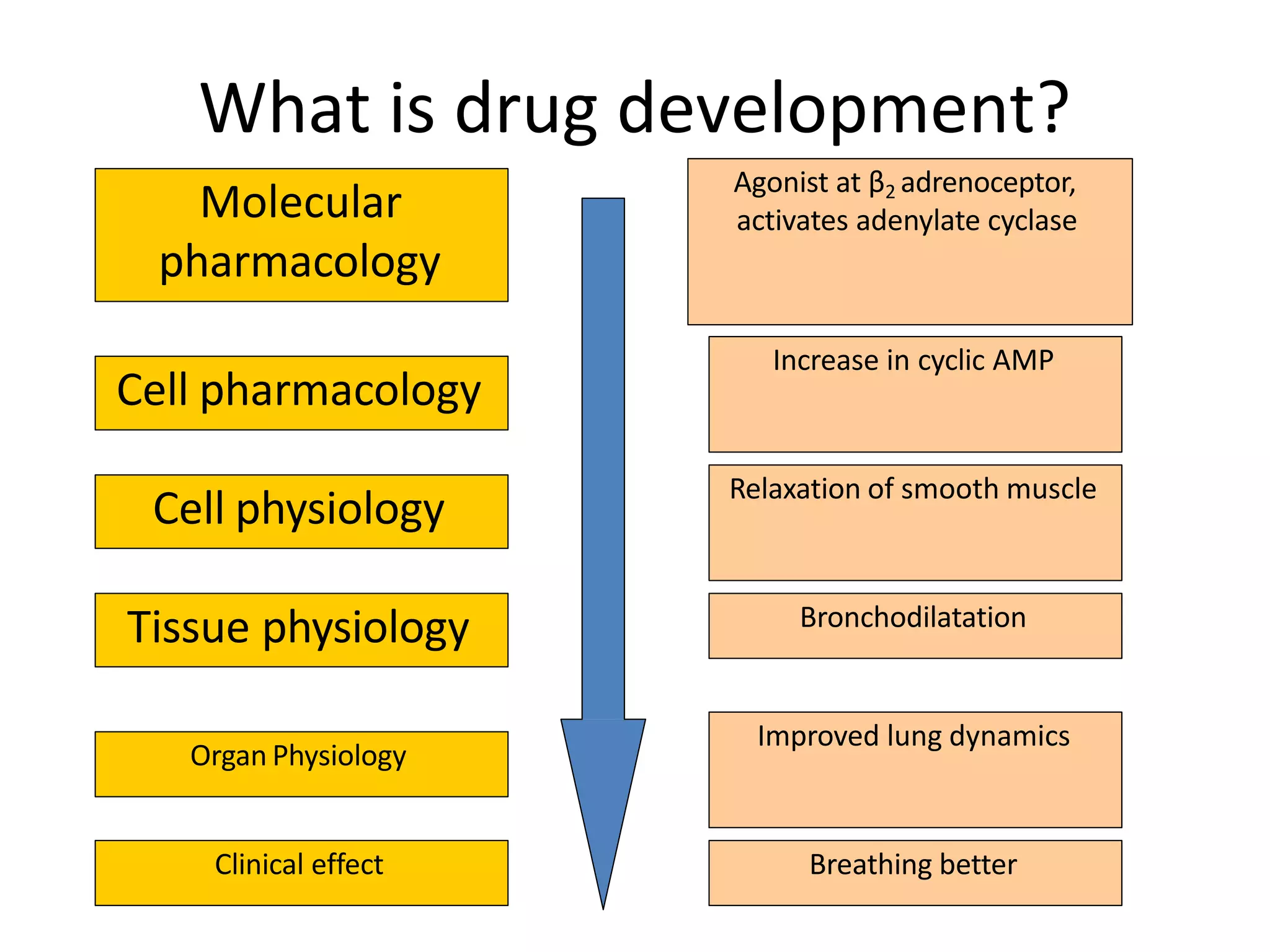
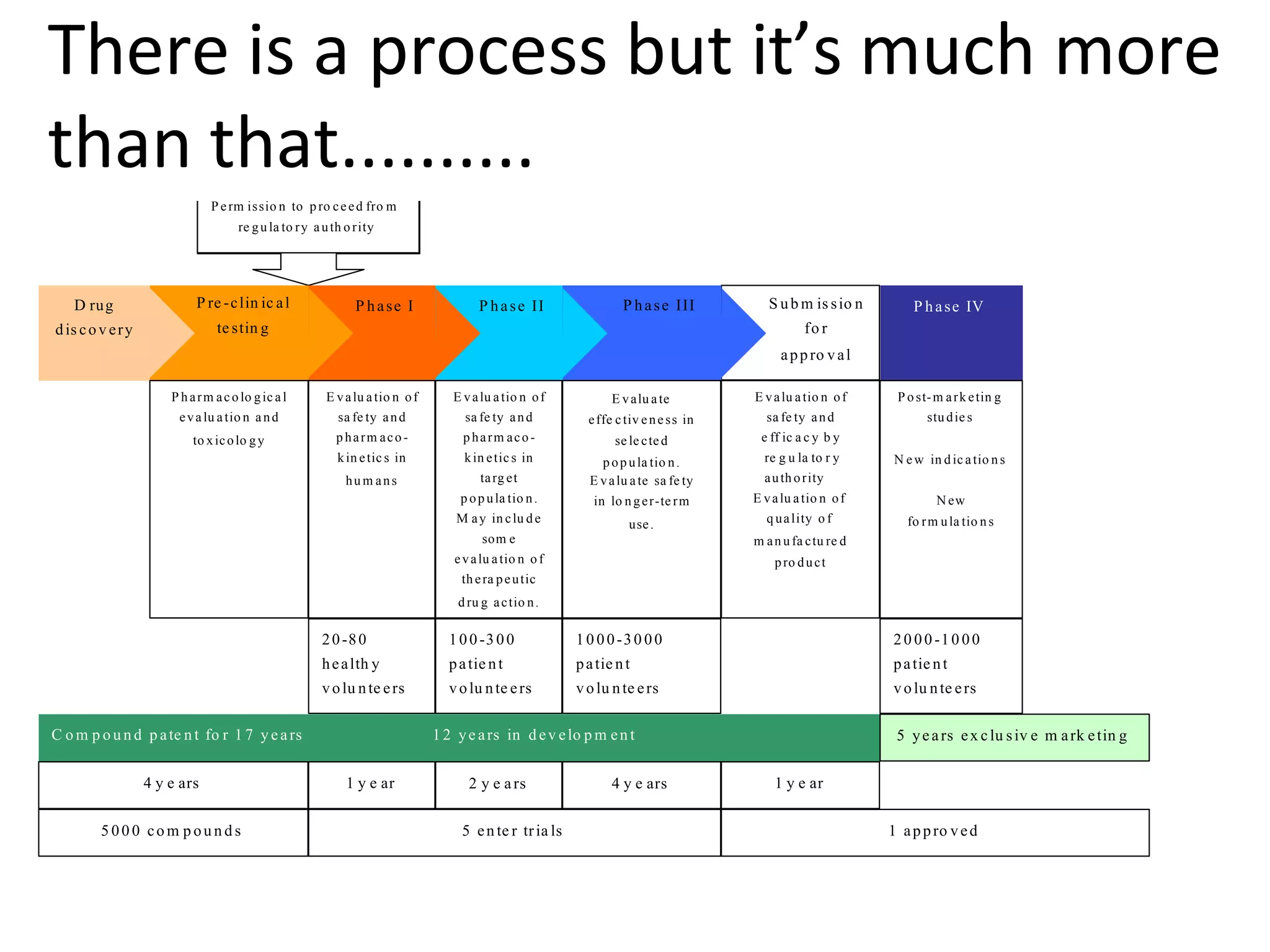
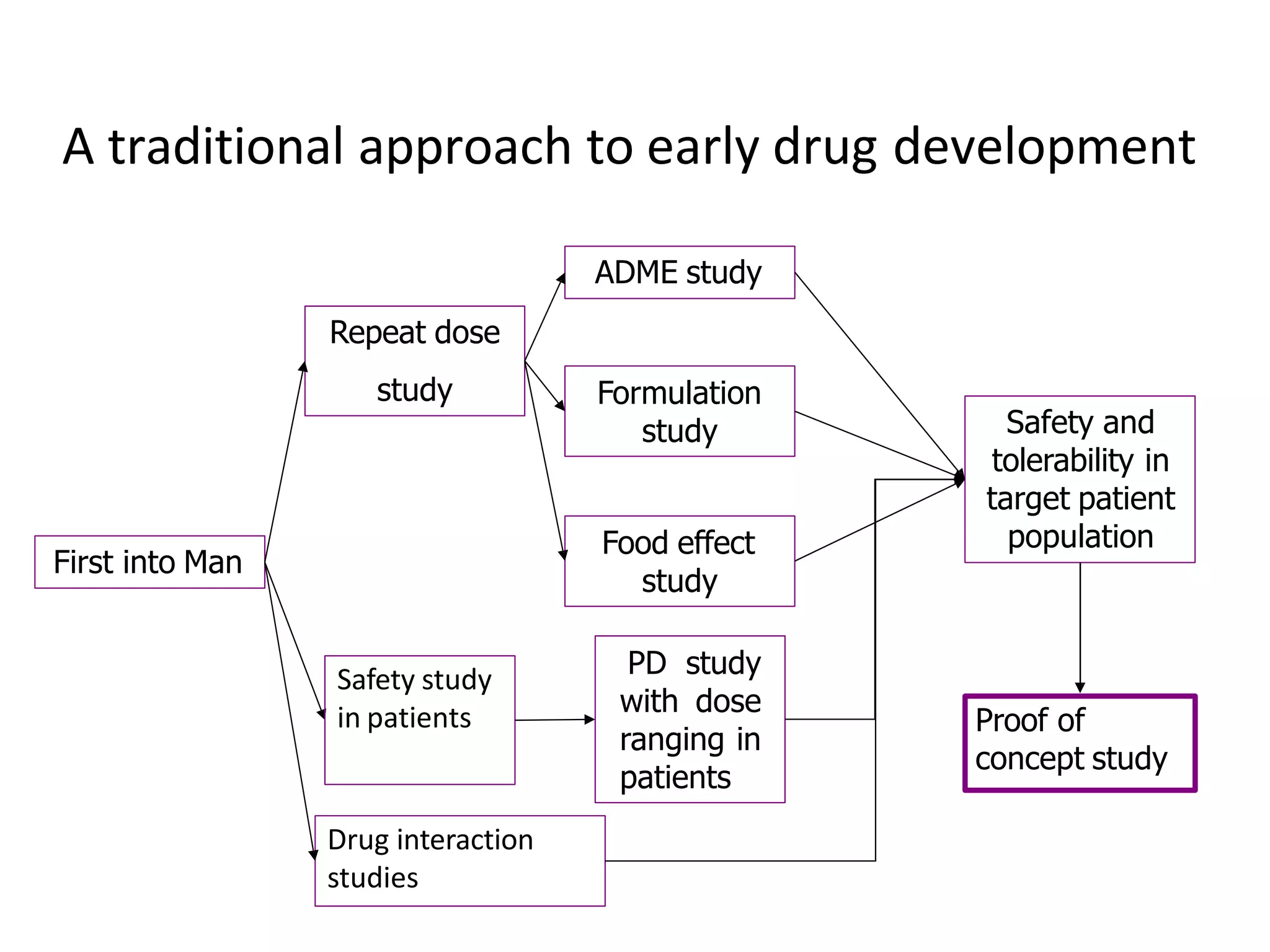
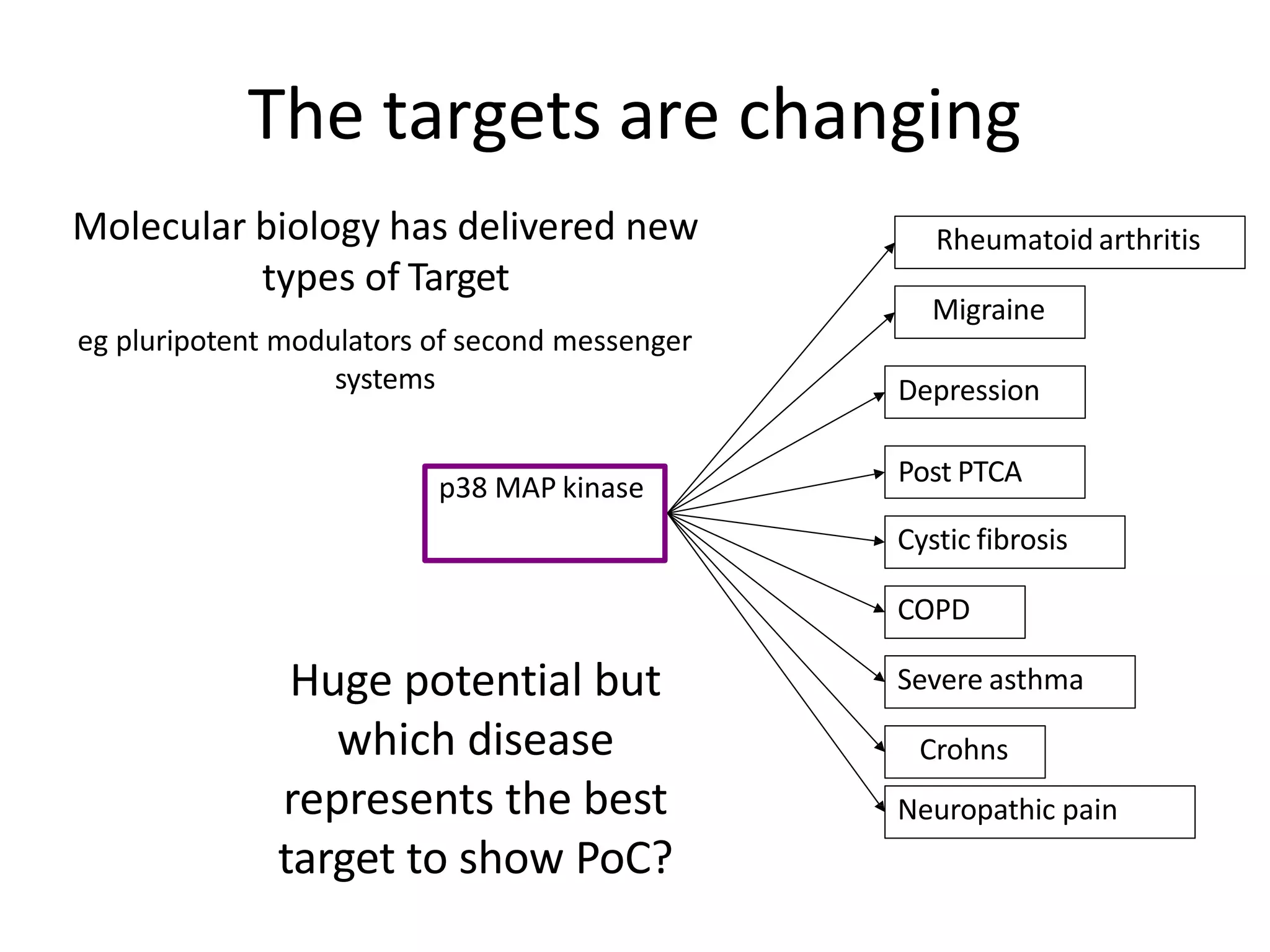
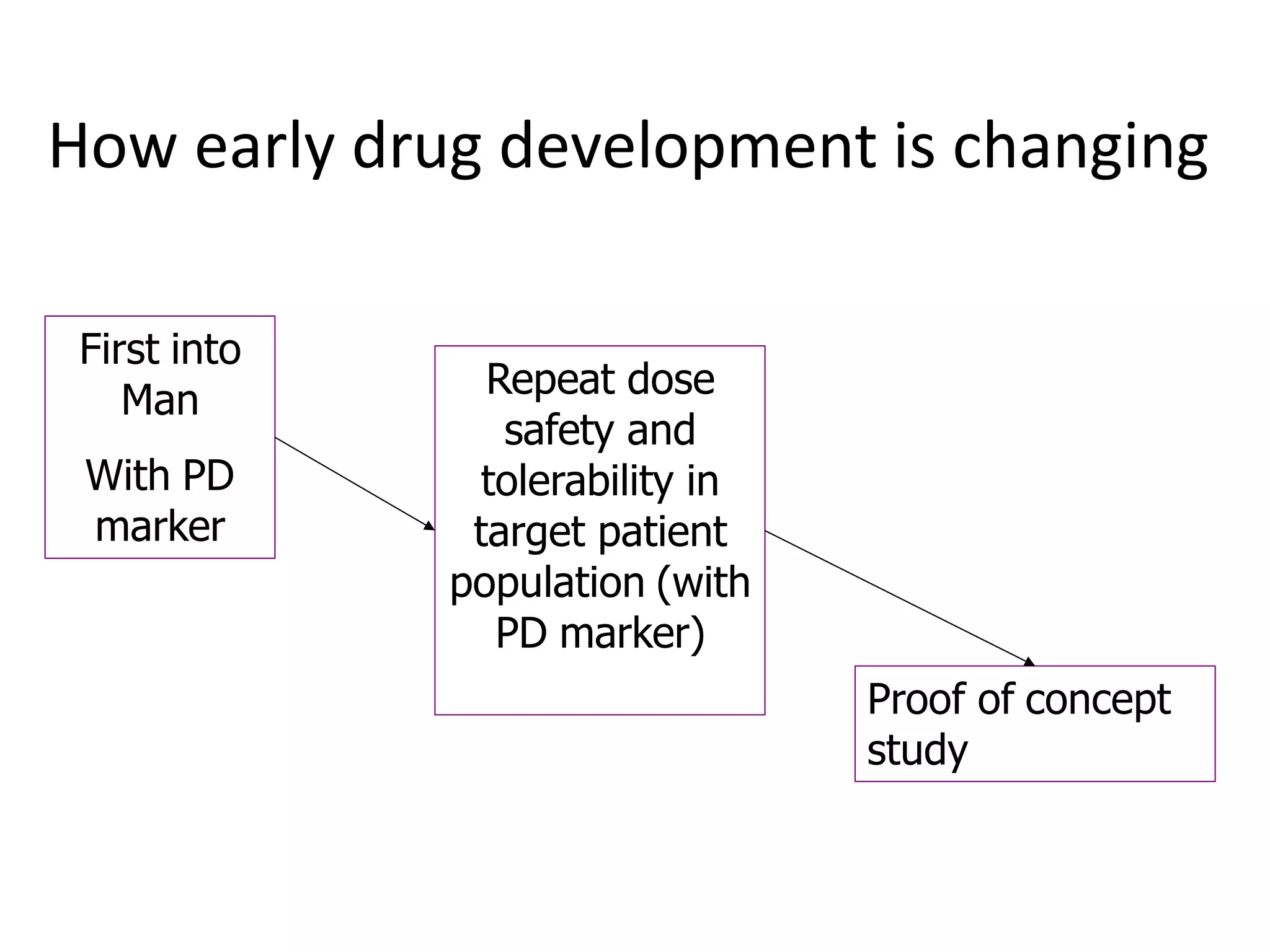
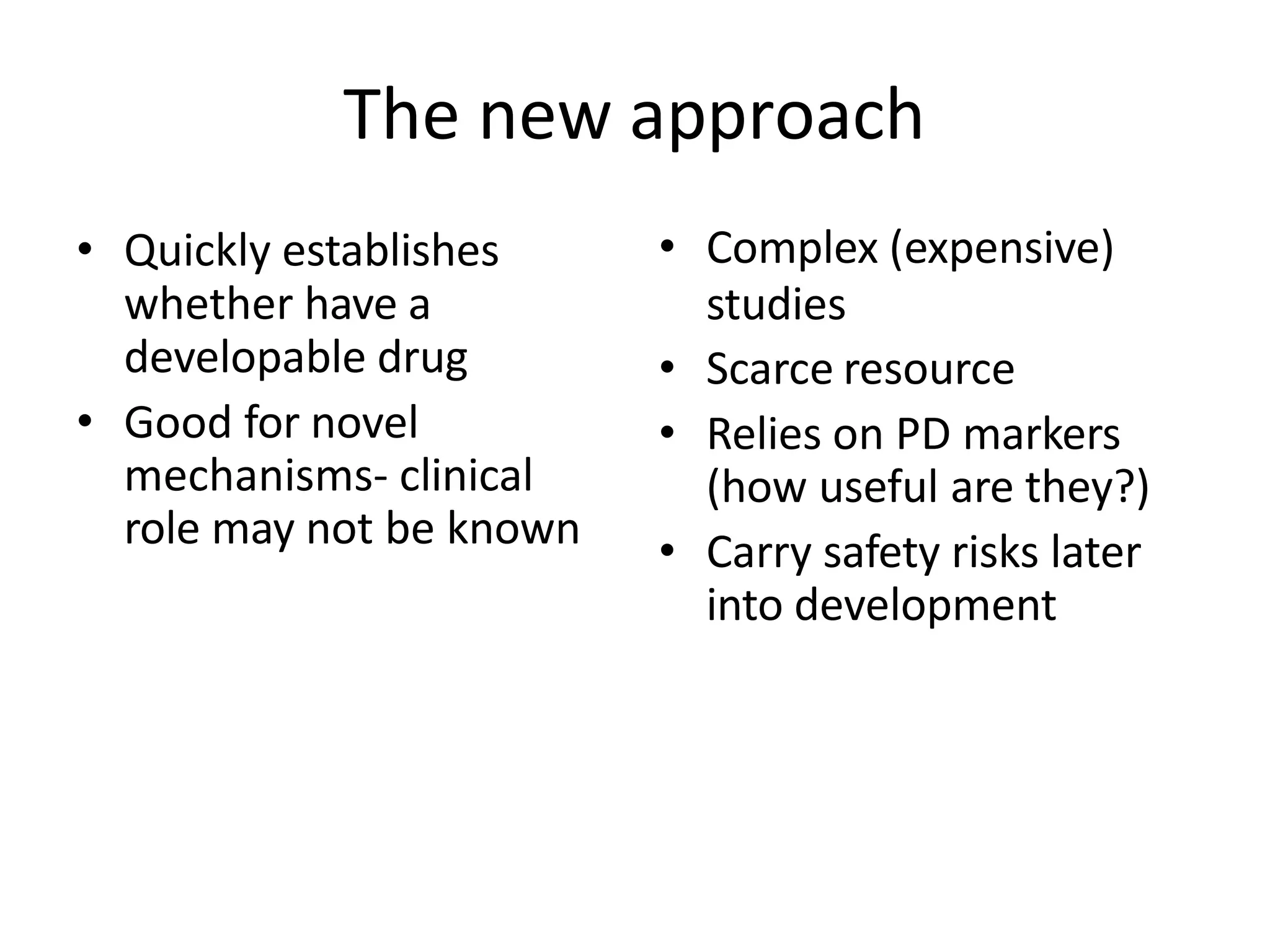
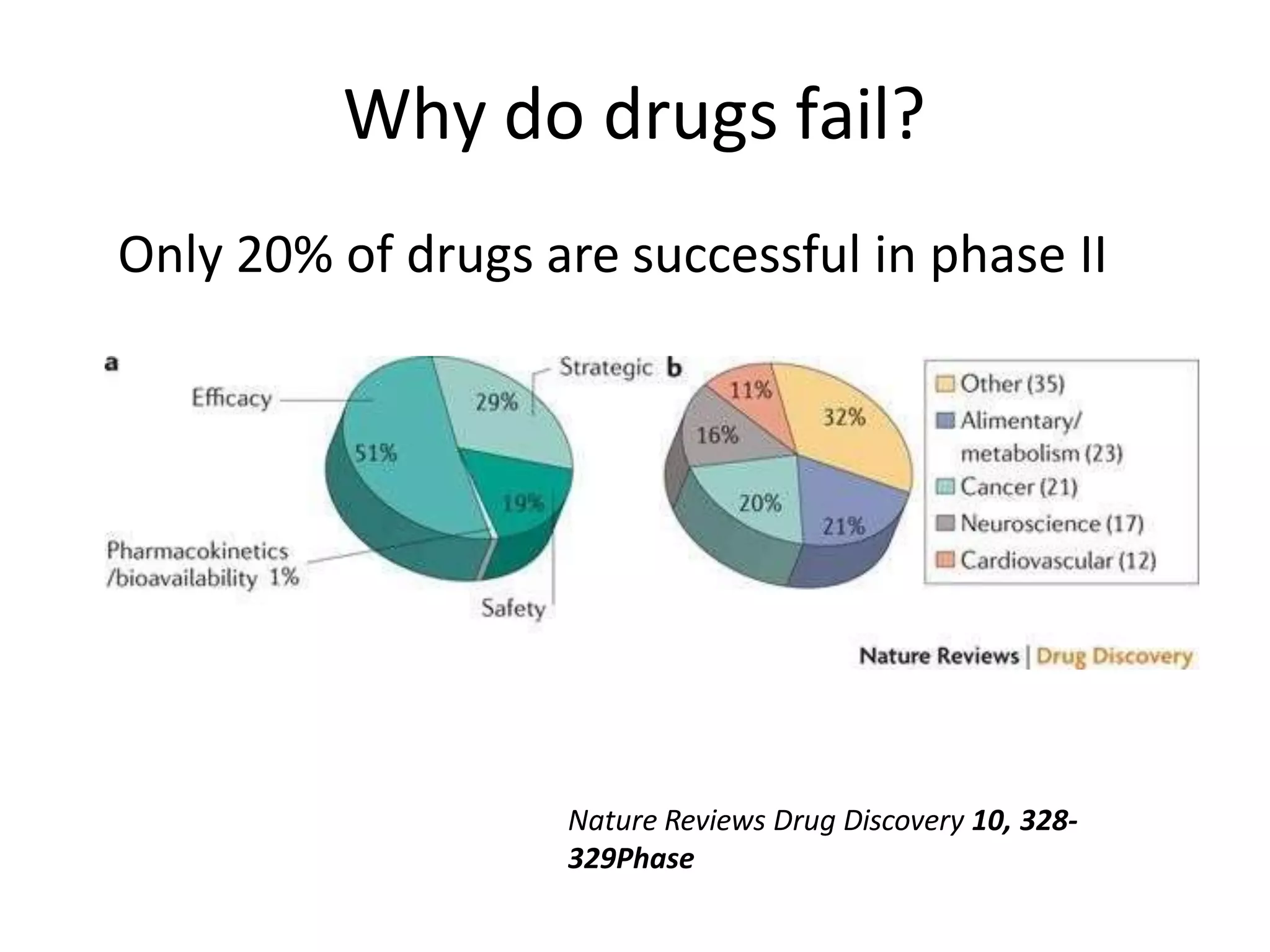
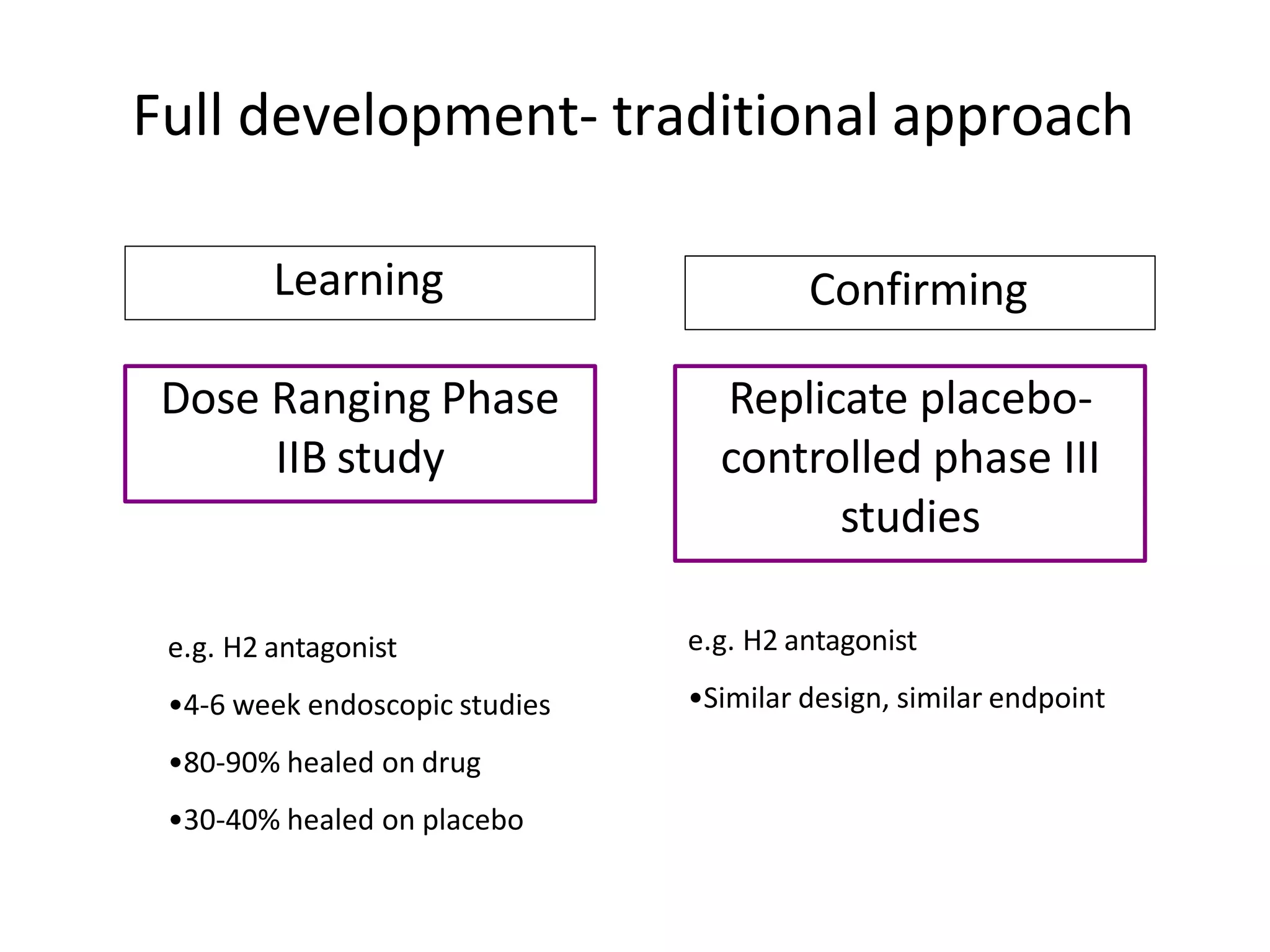
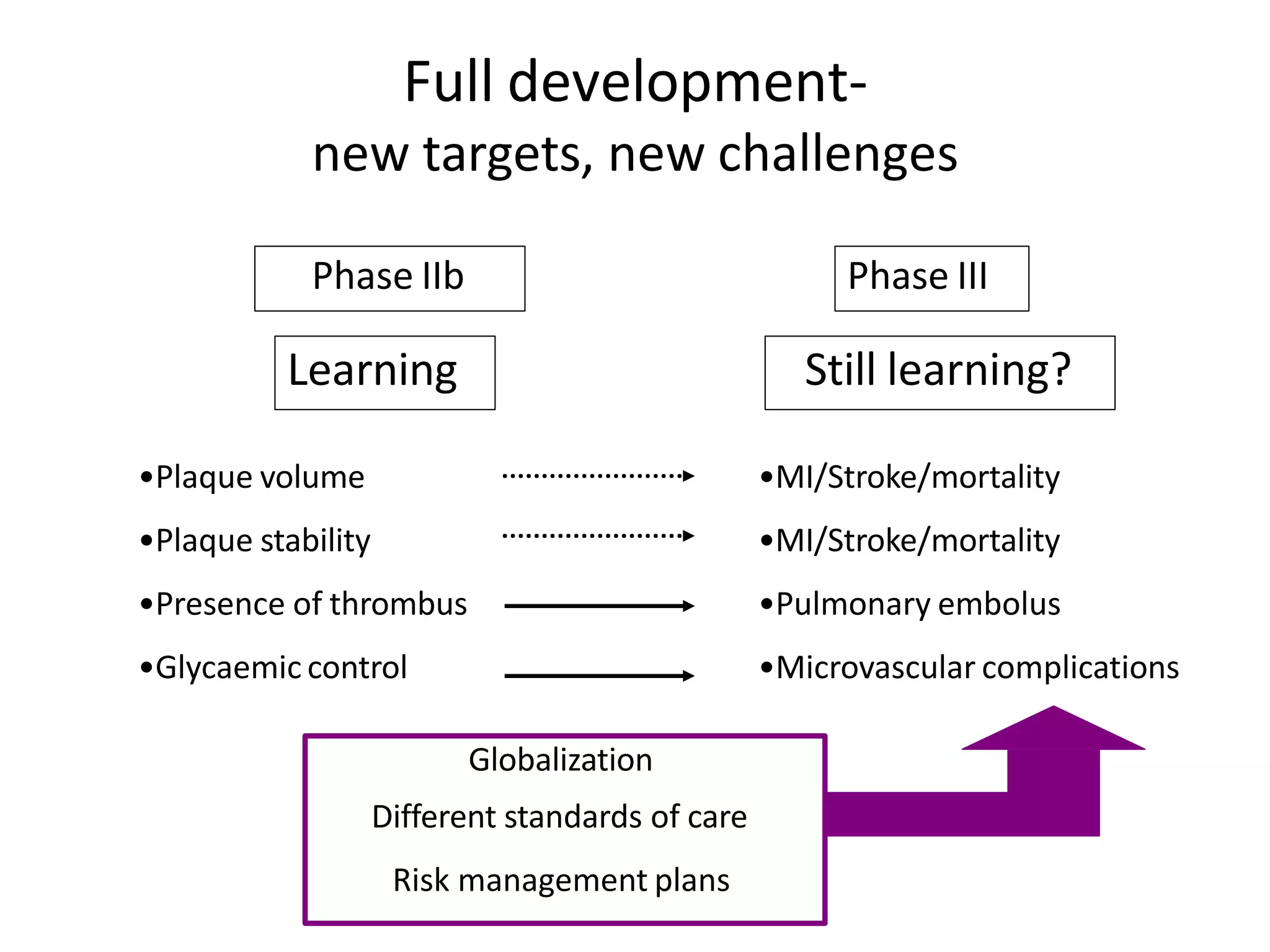
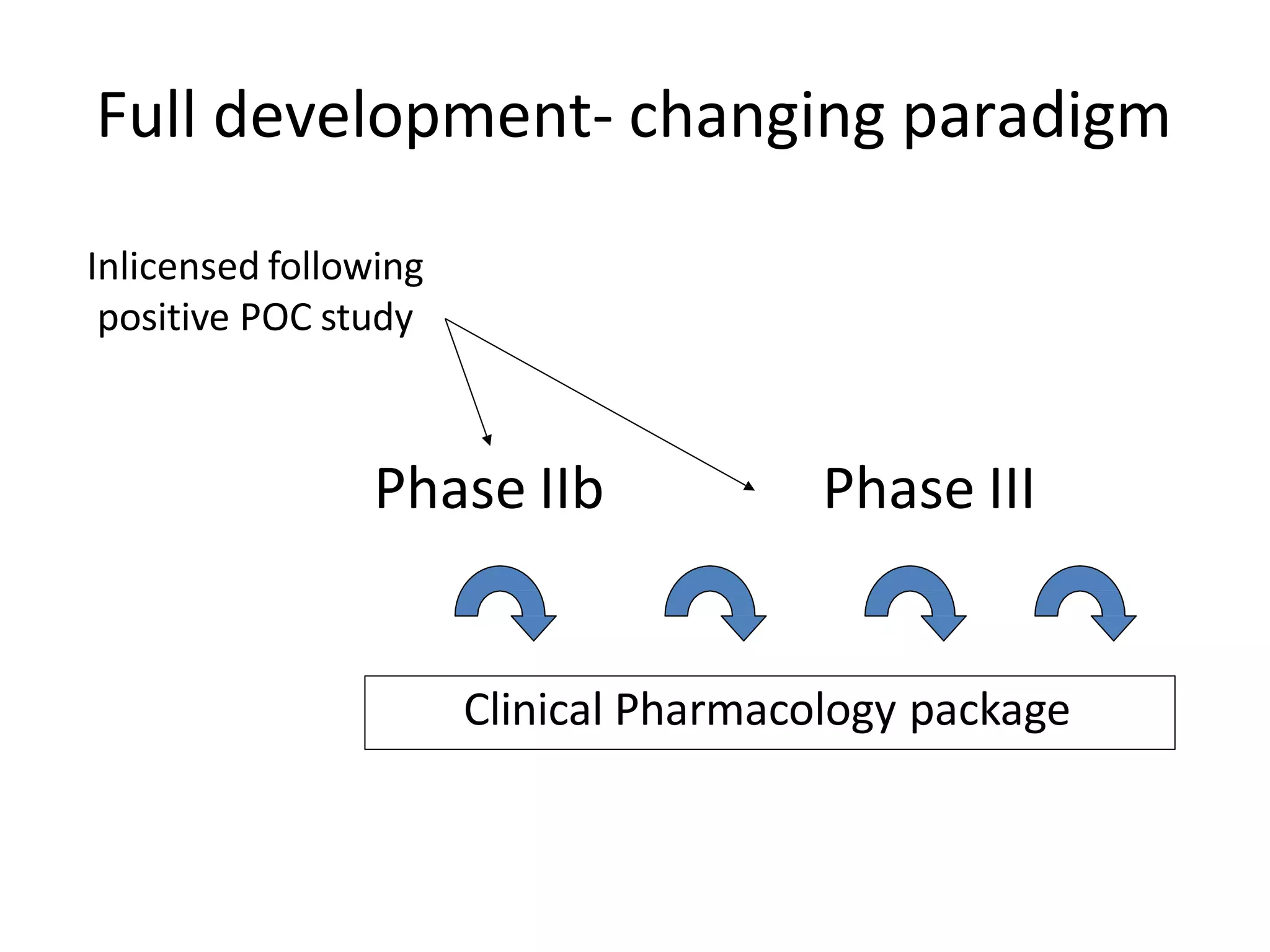
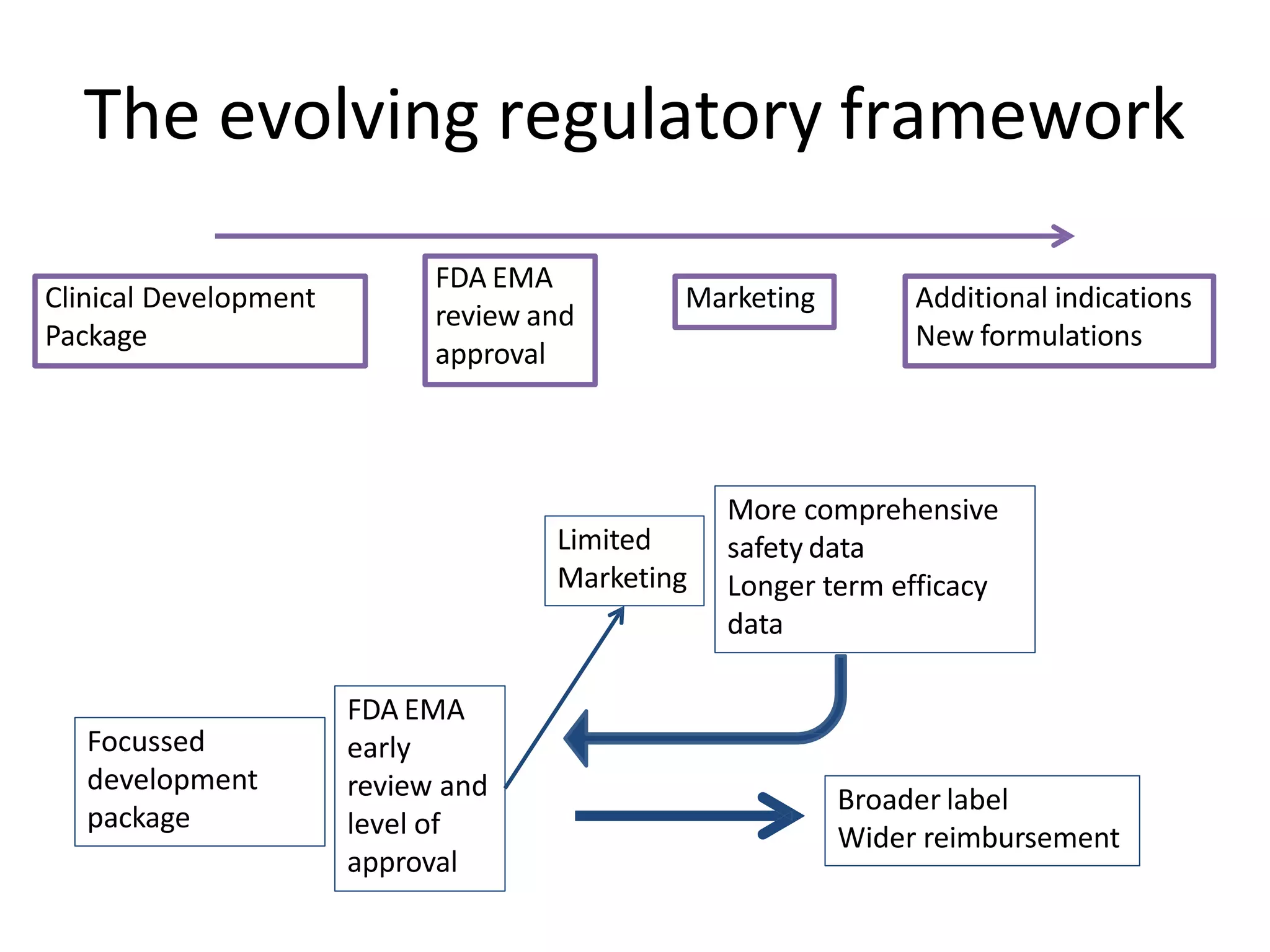
This document provides an overview of drug development, detailing the various phases including drug discovery, pre-clinical testing, and clinical trials. It discusses the importance of understanding the drug's pharmacology, toxicology, target population, and the regulatory framework guiding the process. Additionally, it highlights the challenges and shifts in drug development strategies, particularly with new targets and mechanisms.




























































![Preclinical_Phase_of_Drug_Development_Lucas[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/preclinicalphaseofdrugdevelopmentlucas1-251107071109-7c5cab19-thumbnail.jpg?width=640&height=640&fit=bounds)


















































