
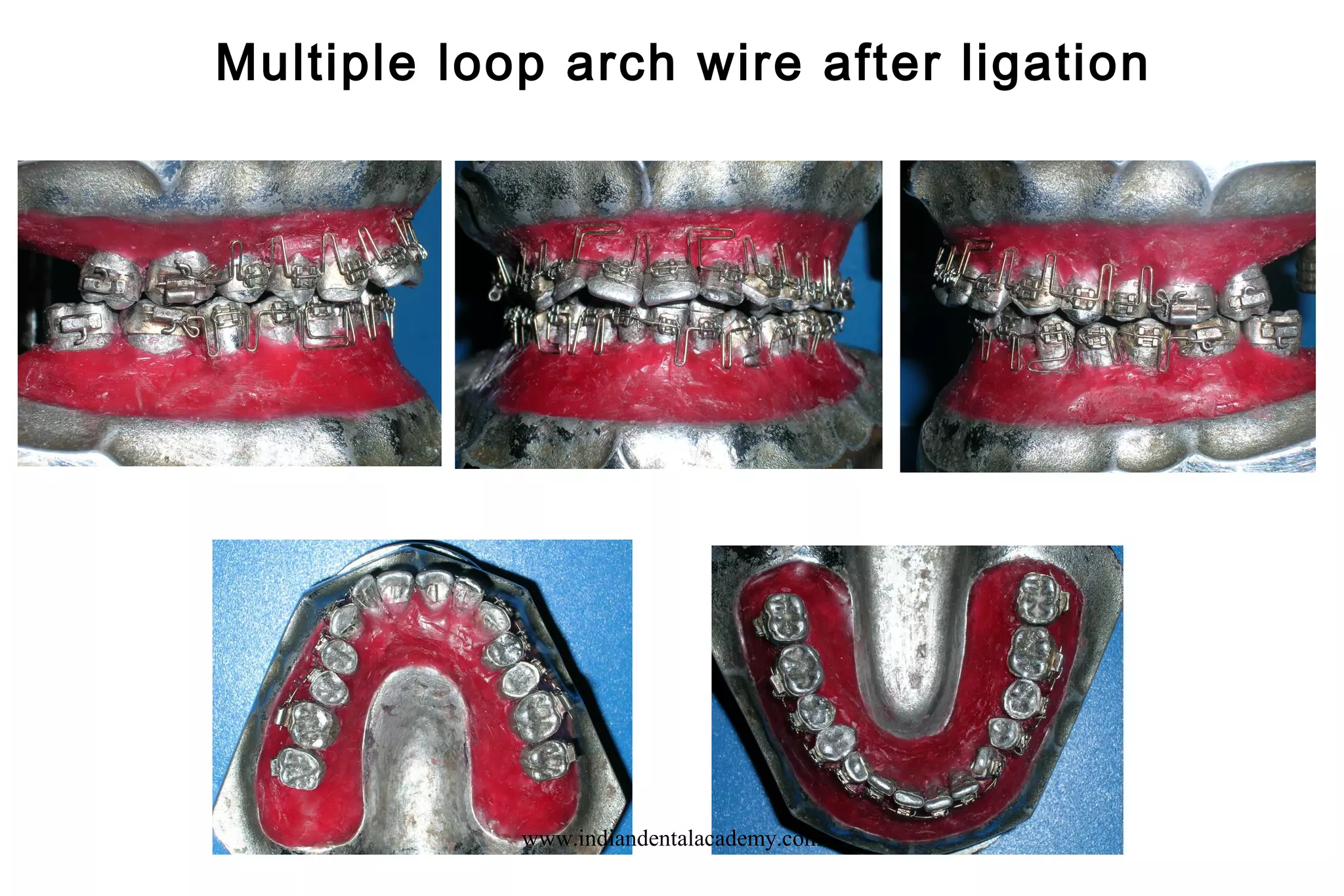
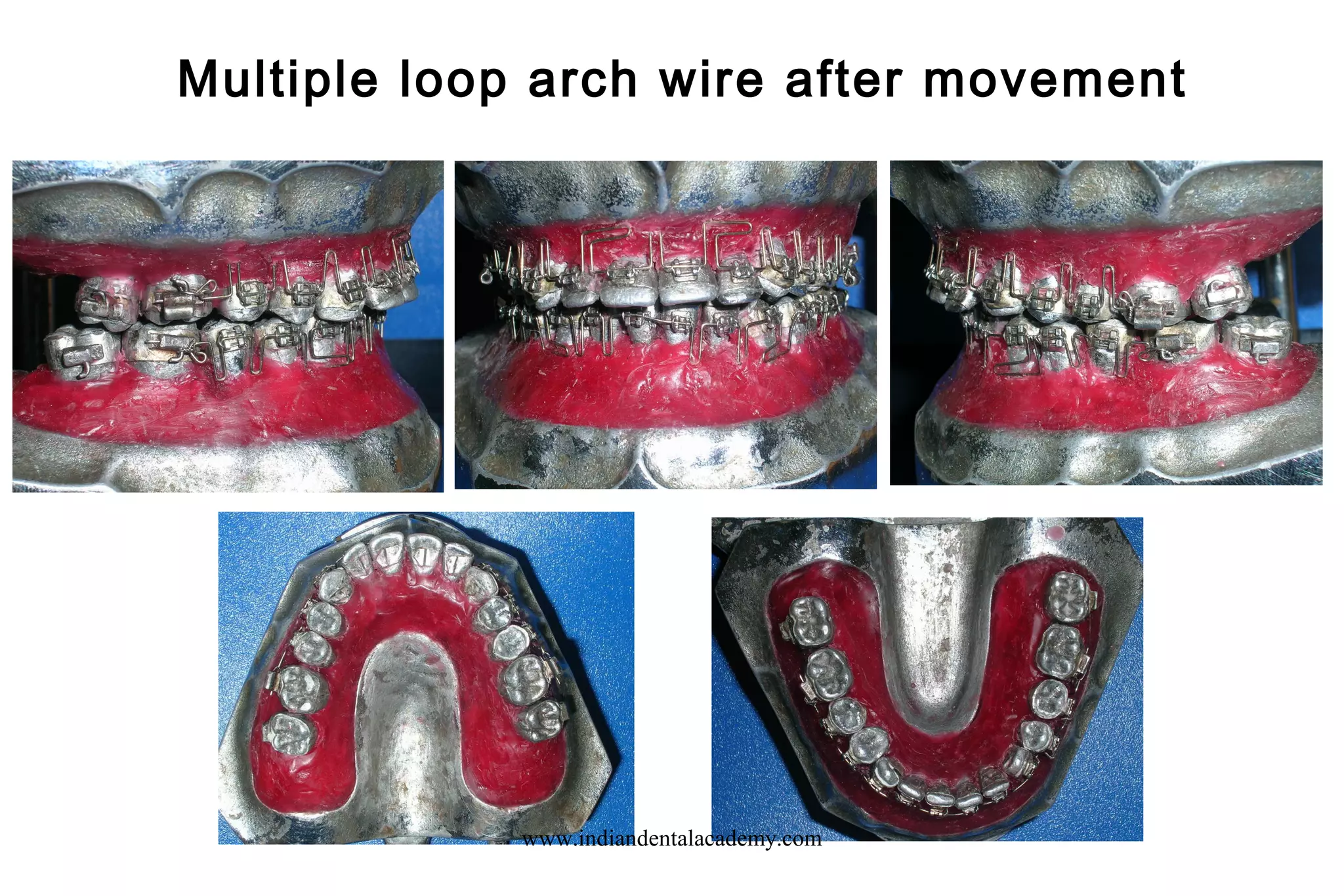
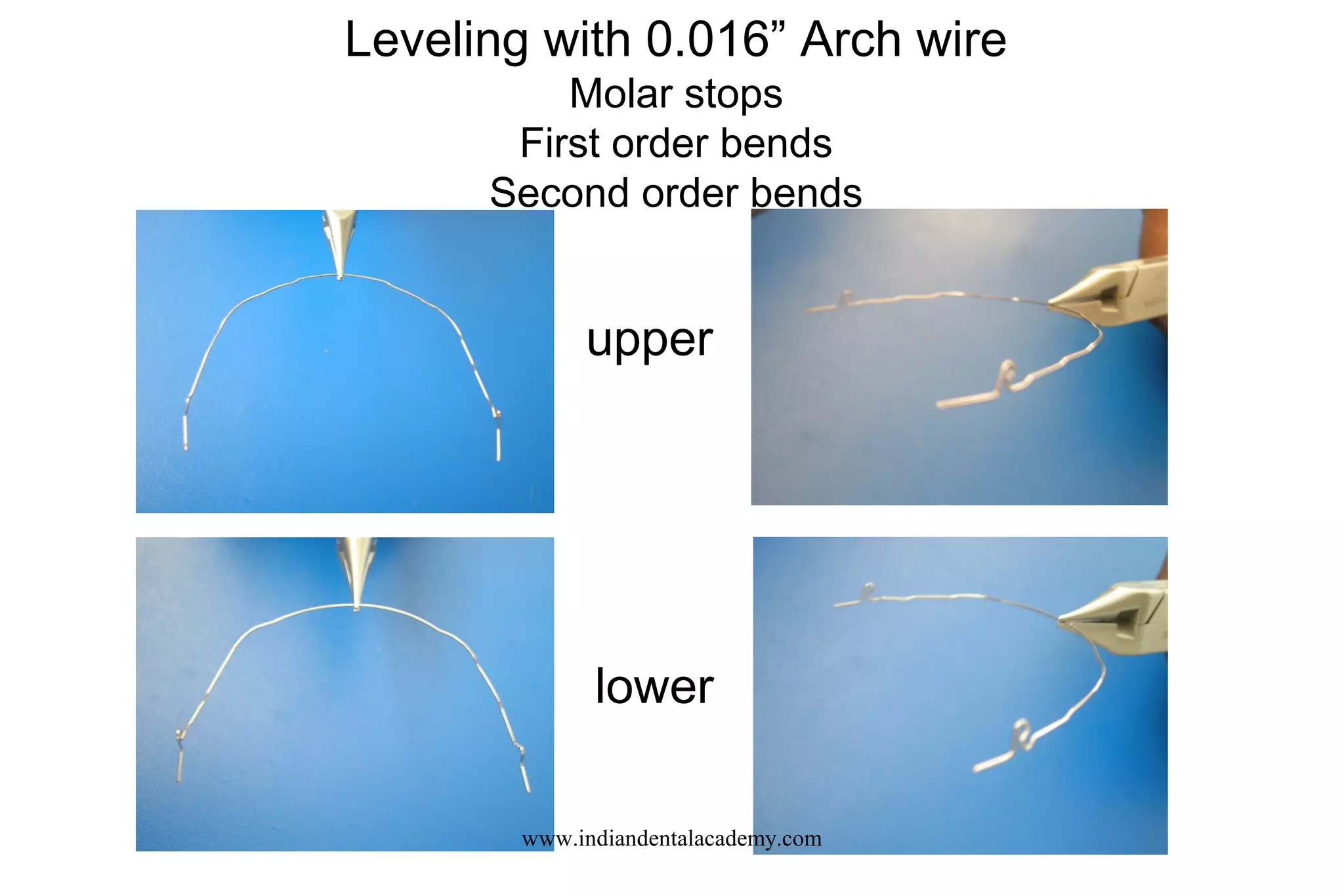
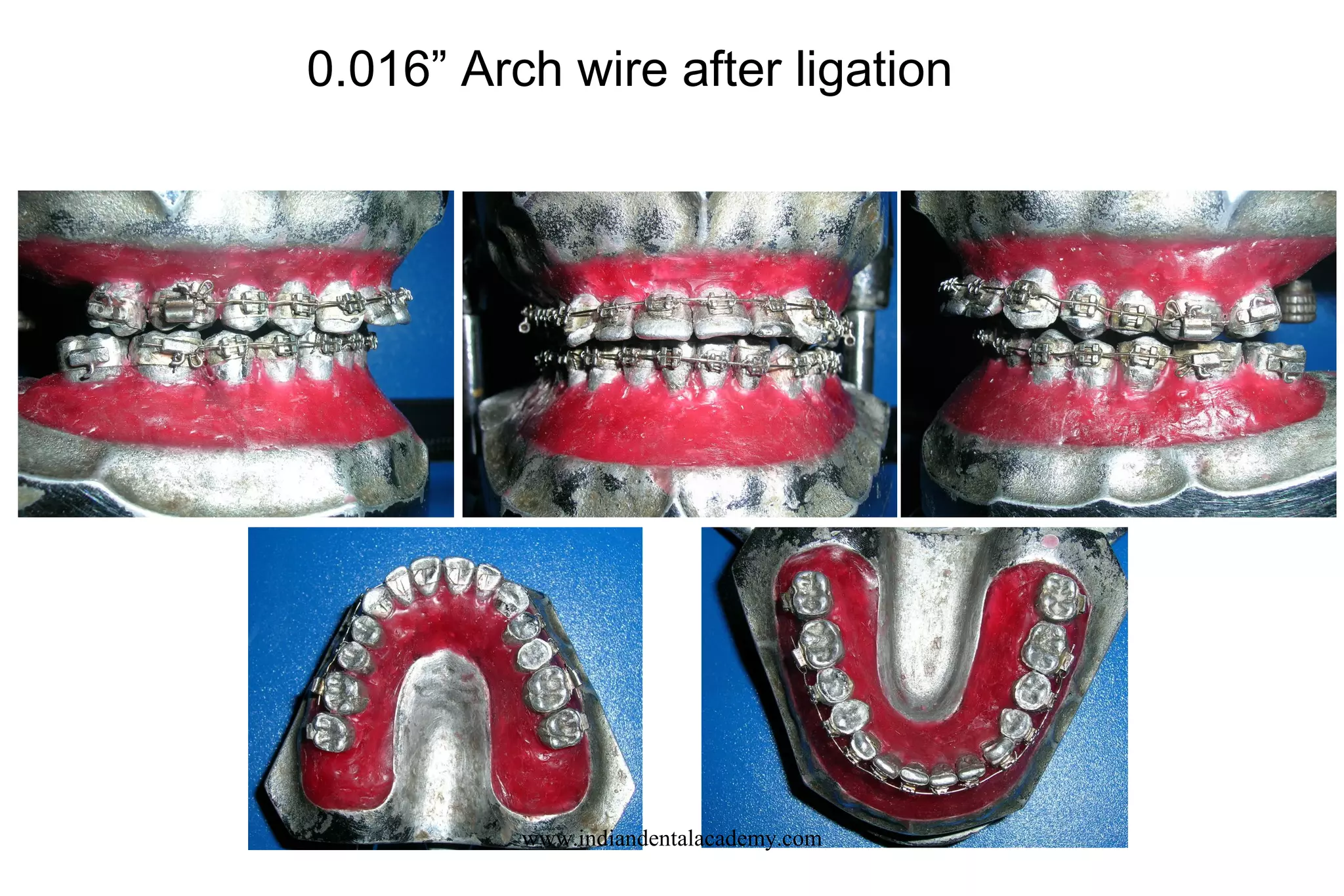































The document discusses various growth trends in orthodontics, specifically type A, B, and C trends affecting facial structure and their implications for orthodontic treatment. It also details the importance of precise bracket placement, techniques for computerized bonding, and principles for alignment arches. Additionally, it covers clinical applications of loop mechanics in tooth movement and emphasizes best practices for orthodontic wire selection and leveling strategies.























































































