Download as PDF, PPTX




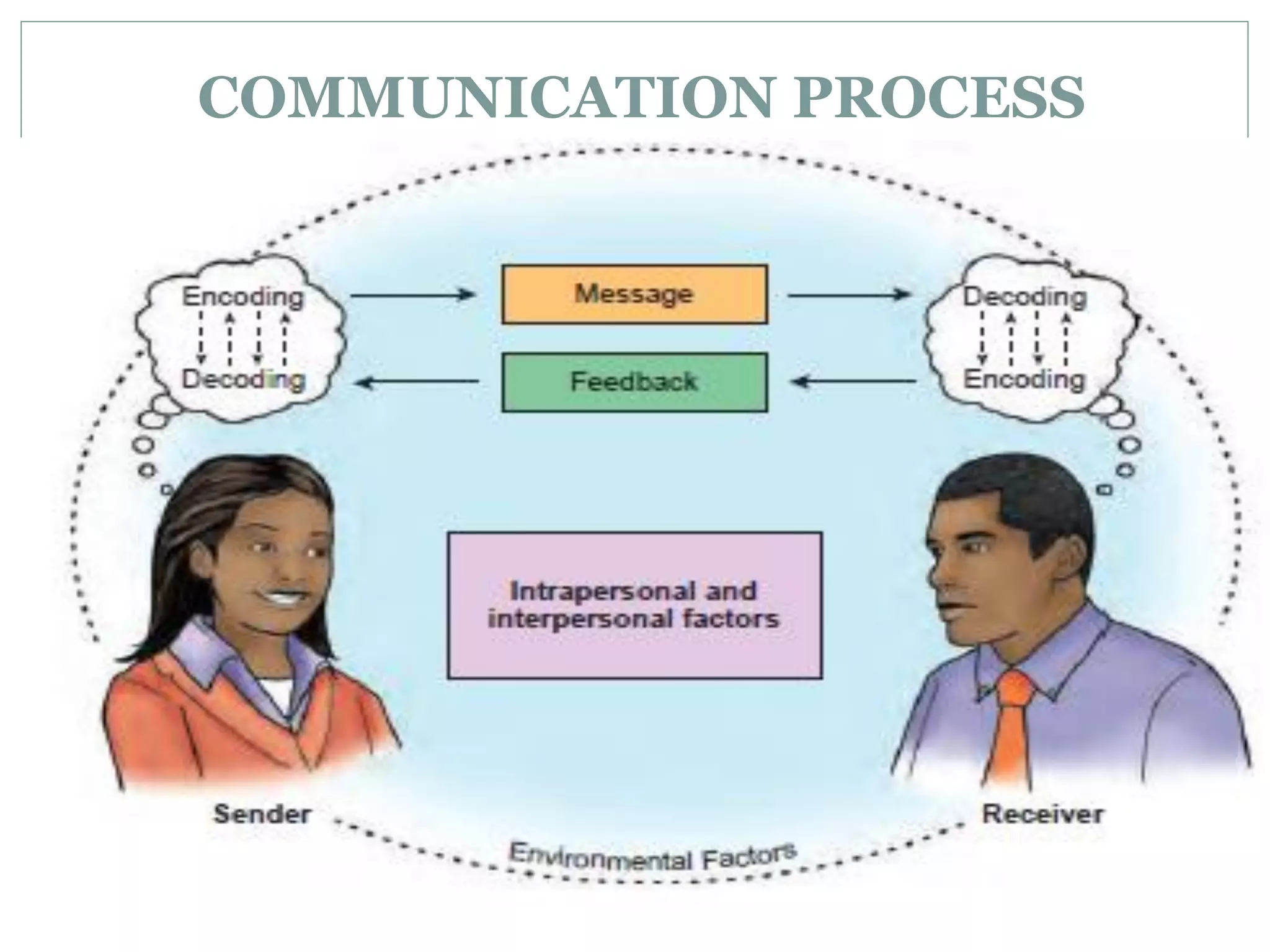

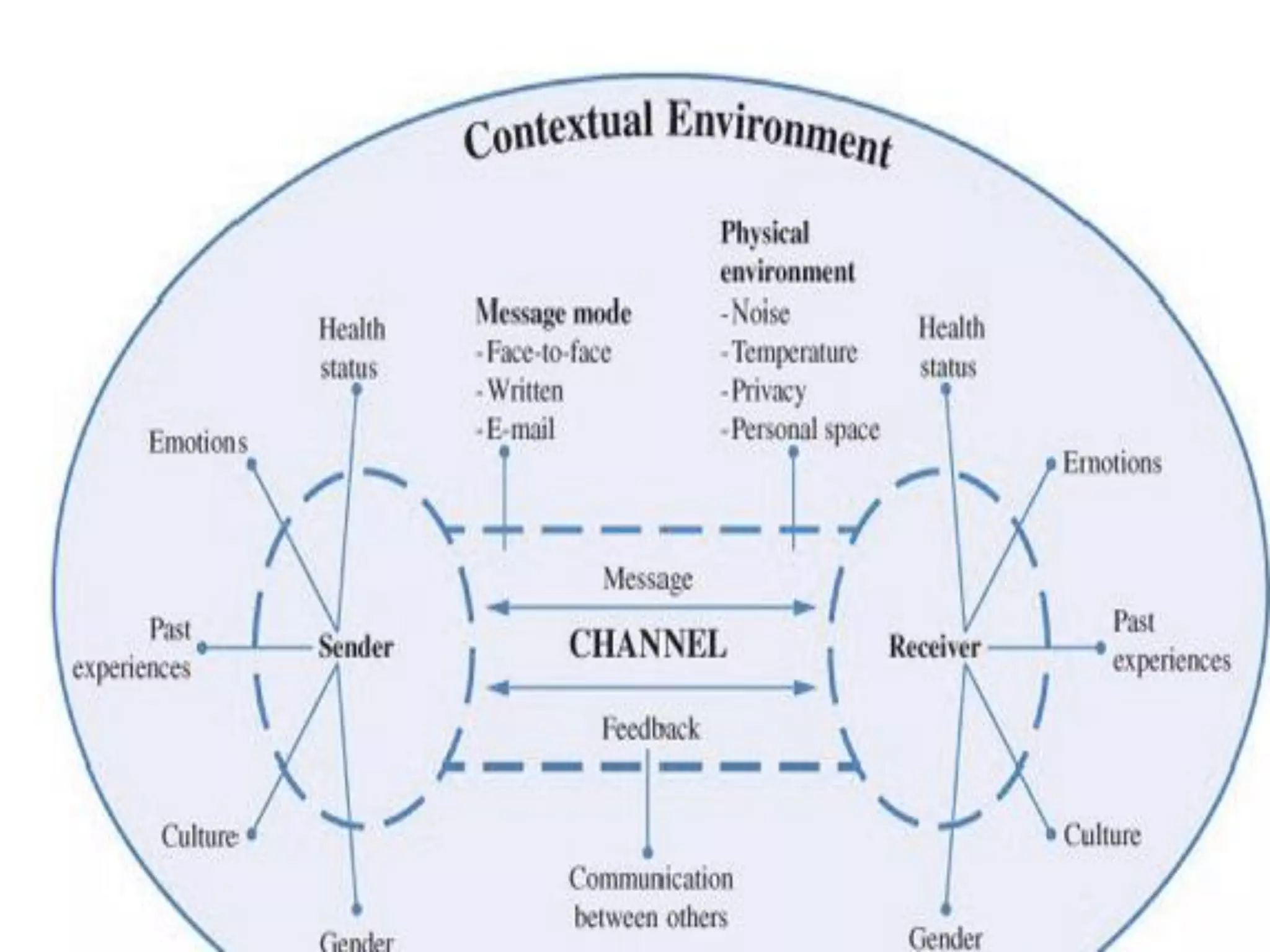














































































This document discusses communication in healthcare. It defines communication and describes its components and process. It discusses different types of communication including verbal, nonverbal, intrapersonal, interpersonal, and group communication. It outlines the sender, message, channel, receiver, and feedback elements of the communication process. It also discusses therapeutic communication techniques used in healthcare to develop trust and show caring. Barriers to communication and factors that affect communication are also summarized.























































































