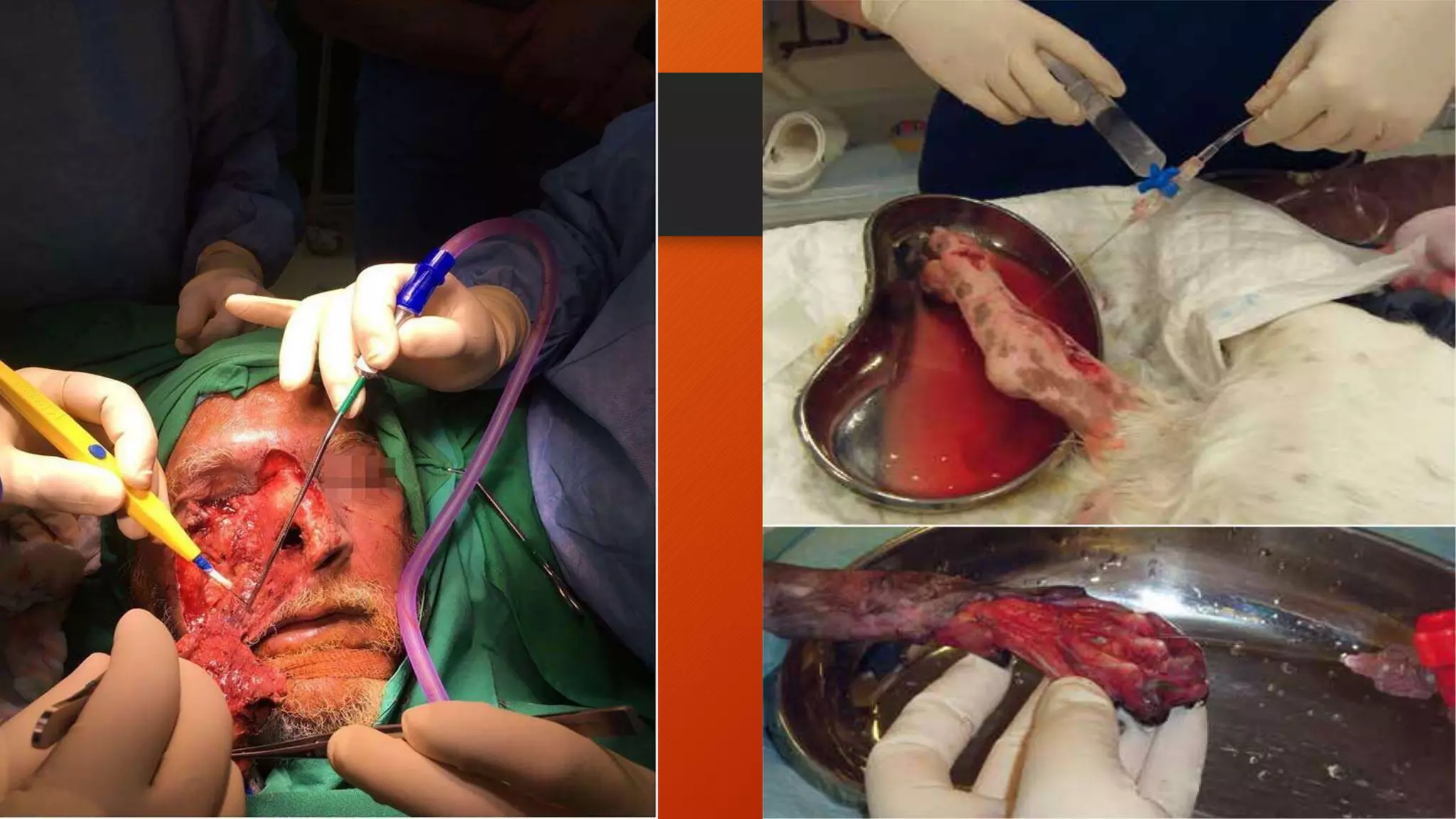
1) A 38-year-old female patient presented with 85% chemical burns following a household accident. She was admitted to the ICU and died 5 days later from complications.
2) The case presentation aimed to provide comprehensive patient care, understand burn disease and management, and develop a nursing care plan.
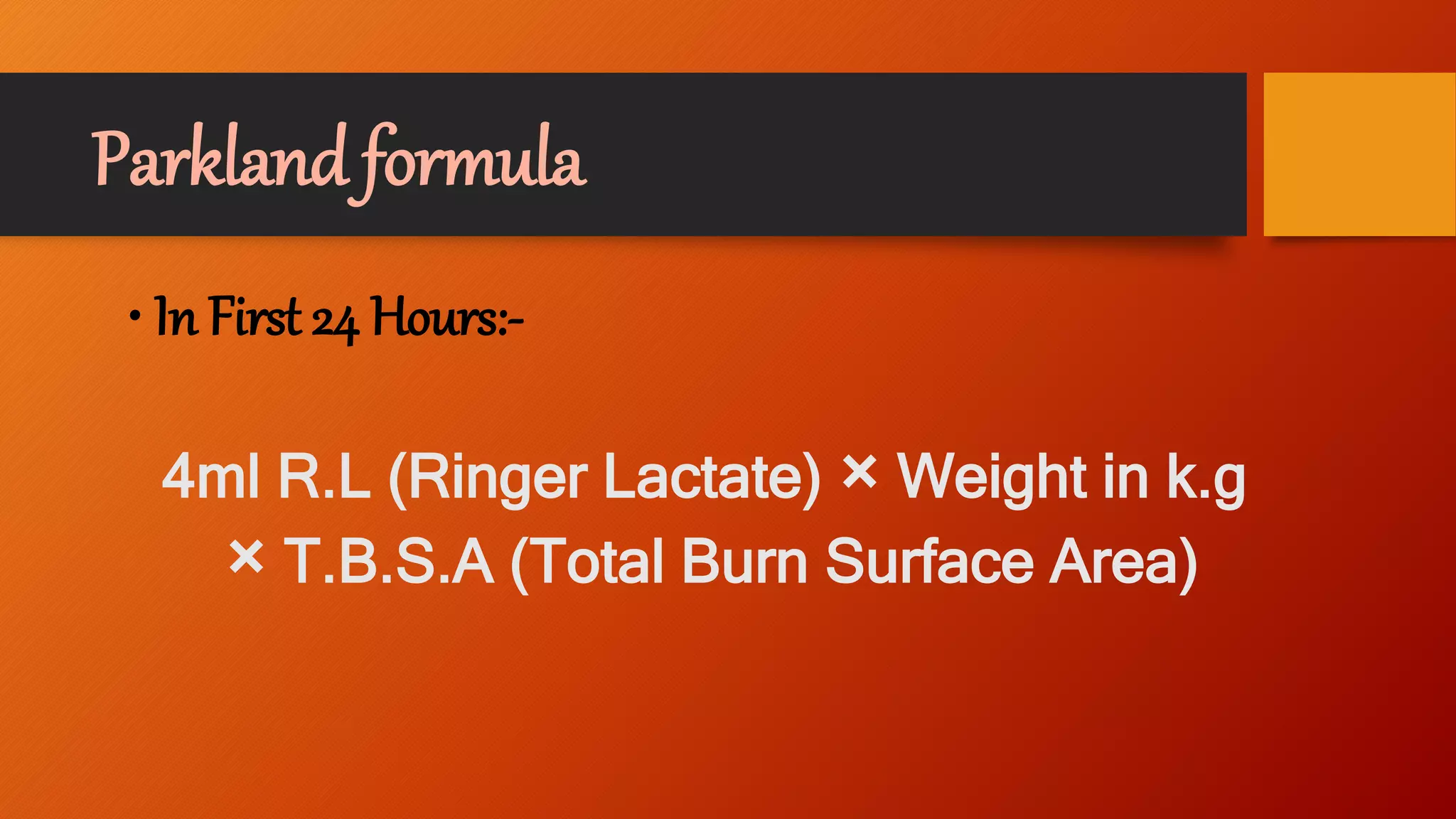
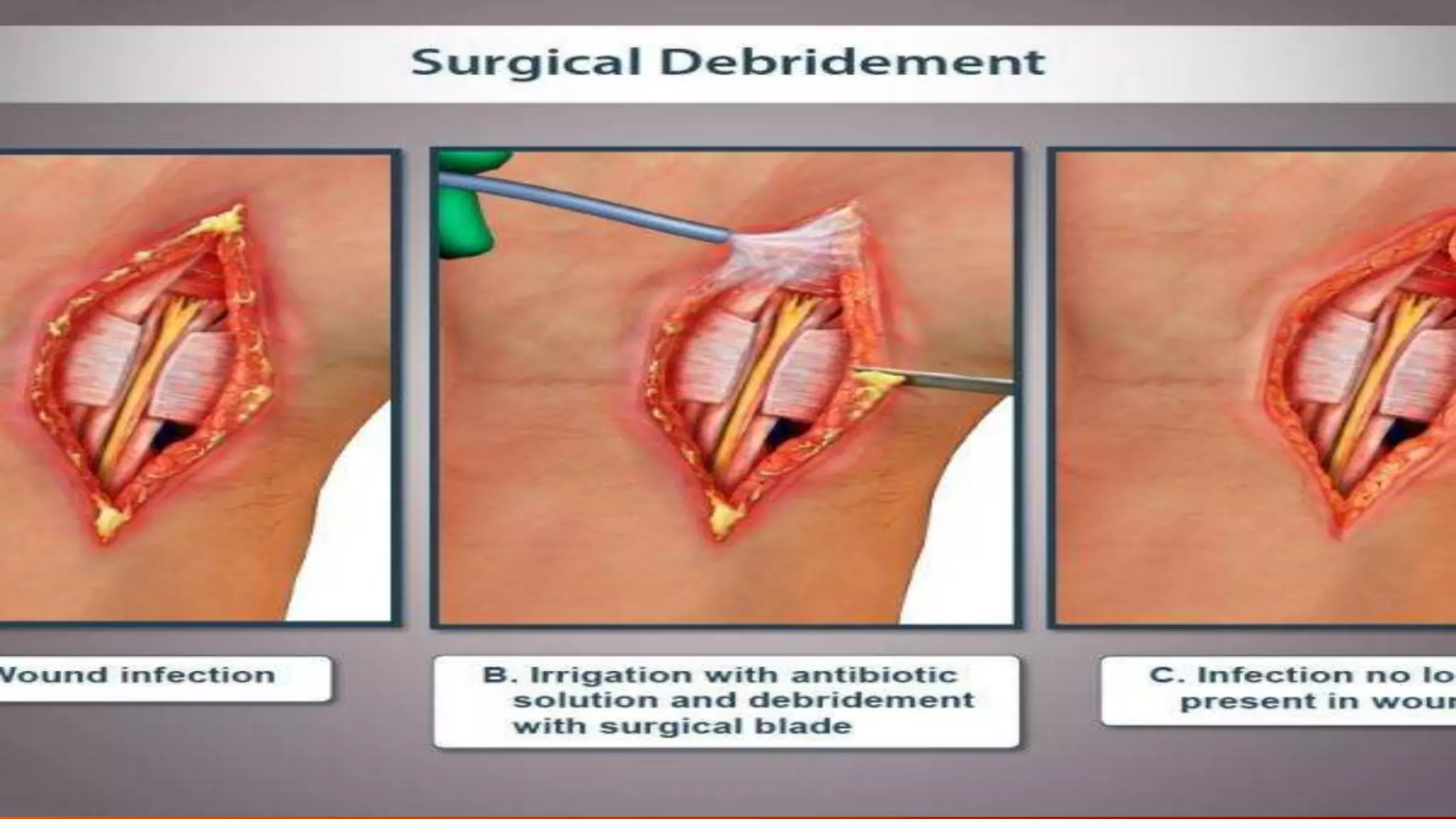
3) Chemical burns can result from strong acids/alkalis and cause severe injury depending on concentration, volume, and contact time with the skin. Management involves fluid resuscitation, wound care, pain management, and rehabilitation. Complications can include shock, infection and organ failure.