This document provides information on various obstetrics procedures and conditions through a series of slides and questions. It discusses amniocentesis, macrosomia, cystocele, perforated uterus, trichomoniasis, ventouse delivery, fetal tachycardia, the menstrual cycle, endometriosis, shoulder presentation, precocious puberty, galactorrhea, ectopic pregnancy, pelvimetry, PCOS, anencephaly, facial palsy, and C-section. Key points covered include indications, risks, diagnostic findings, and management approaches for each topic.
Qs:
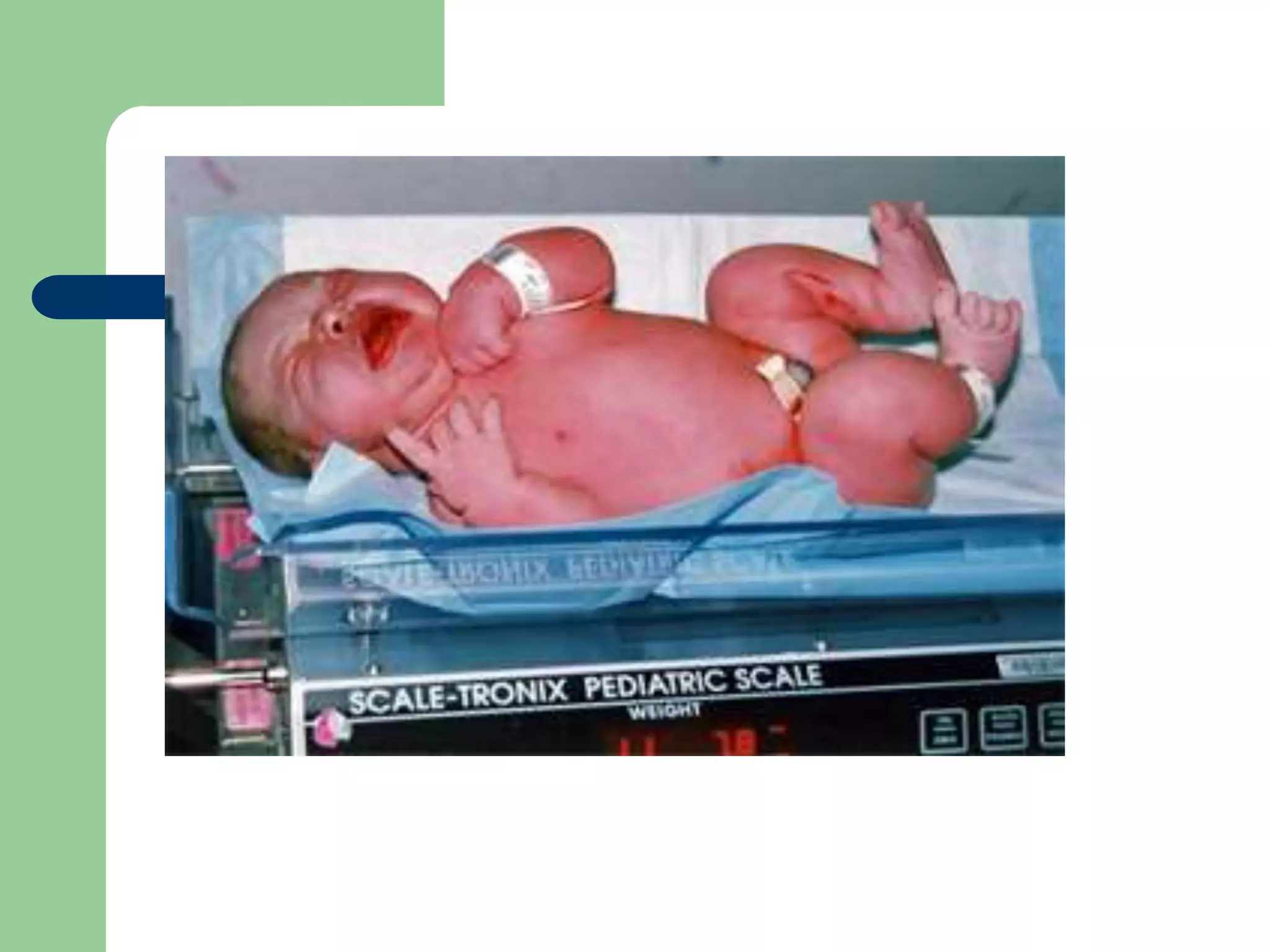
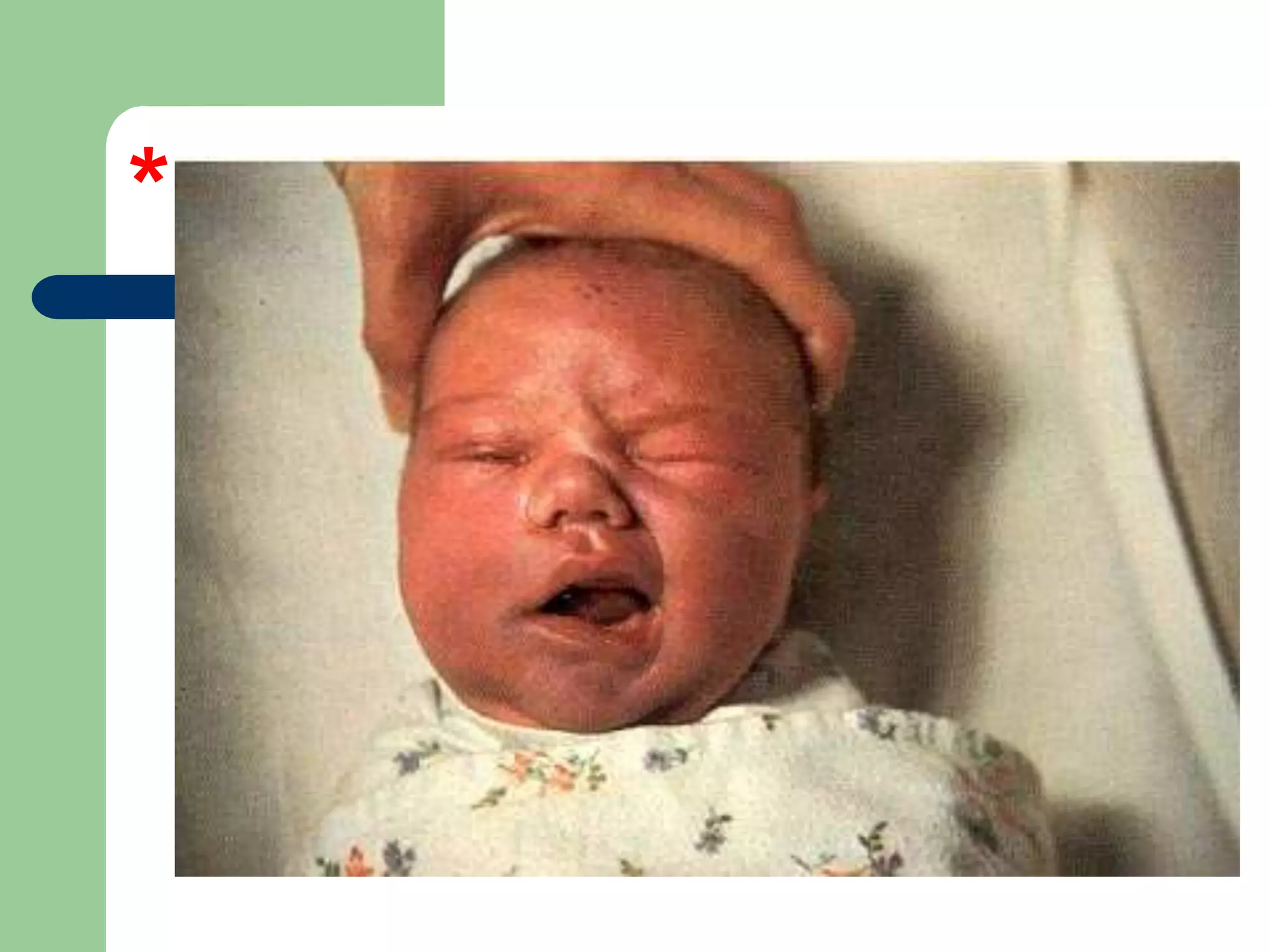
What isthis condition?
Name 4 causes.
Which of them has highest dangerous
complications. And why?
Name 2 complications you would anticipate.
10.
1. Macrosomic baby
2.Diabetic mother (GDM or pre-existing)
Post date
Family history of big babies
Undiagnosed DM
Obese mothers.
Gaining a lot of weight during pregnency.
11.
3.Diabetic mother, becauseit is associated with
fetal poor health and delayed lung maturity
and respiratory distress.
4.Complications:
Polycythemia, hypoglycemia,
hyperbilirubinemia, delayed lung maturity,
shoulder dystotia, prolonged labour and risk
of fetal distress.
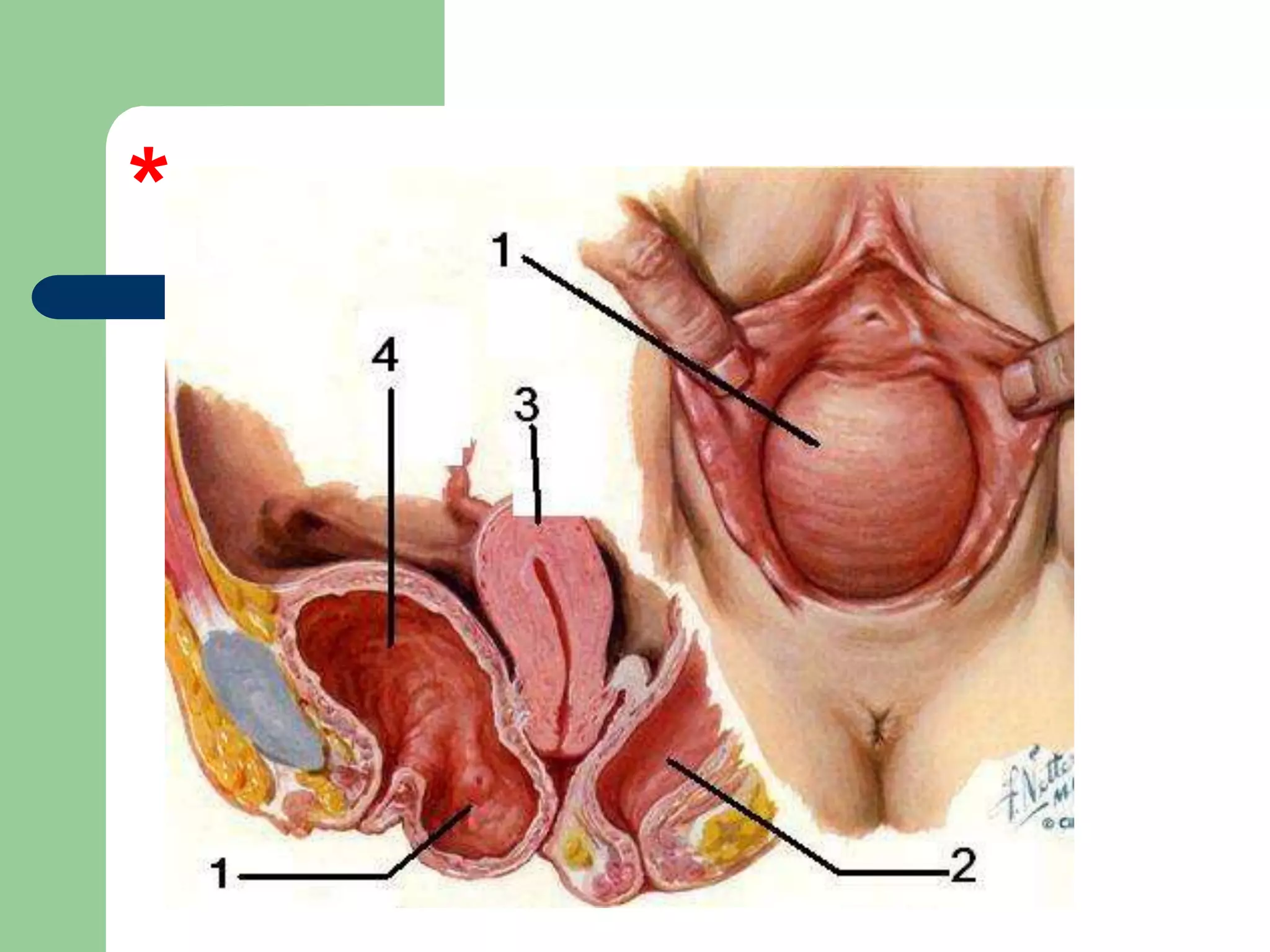
Qs:
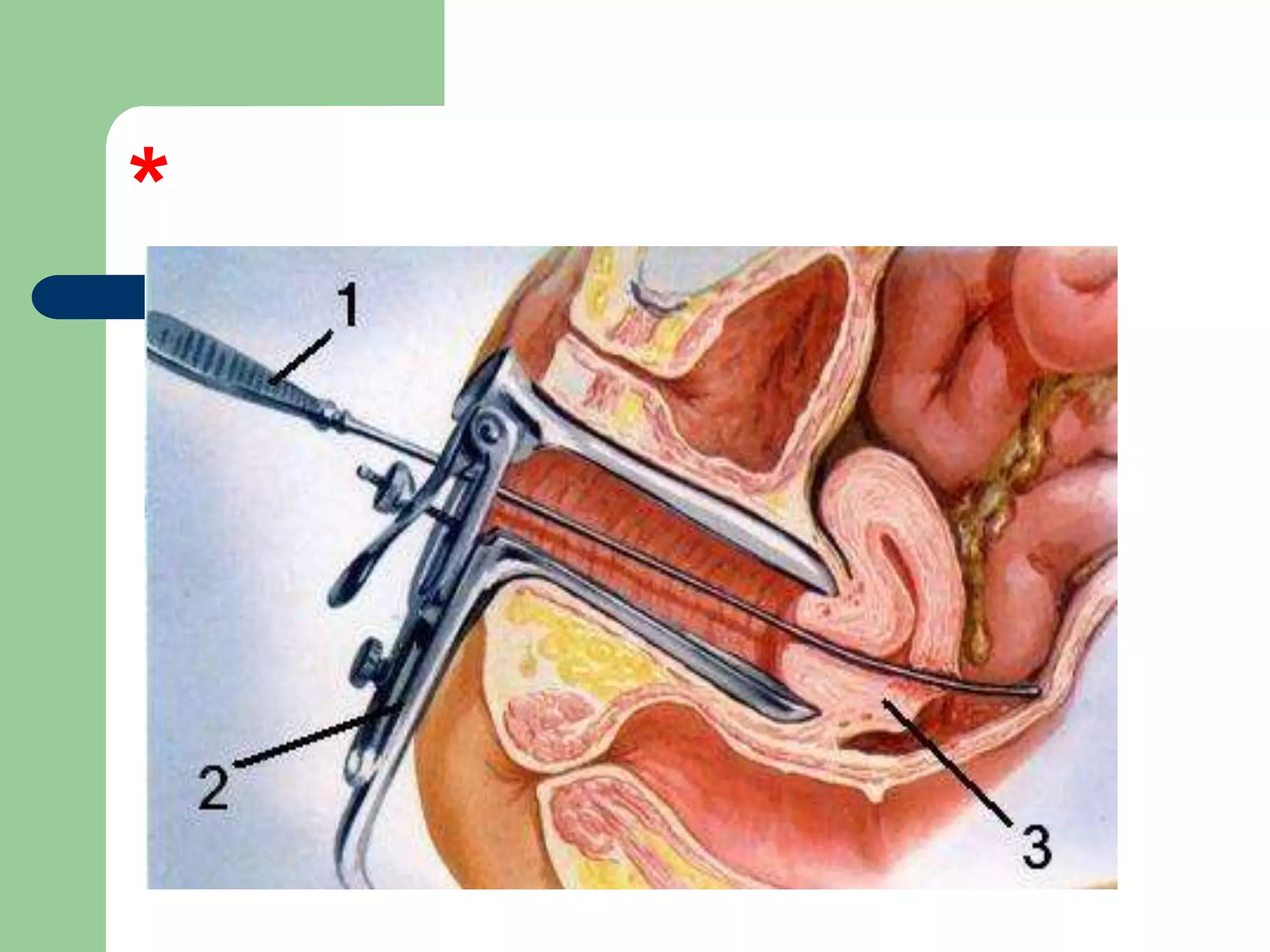
What isthe defect in arrow 3?
What is the position of this uterus?
Identify instruments in arrow (1, 2).
How can you prevent this condition.
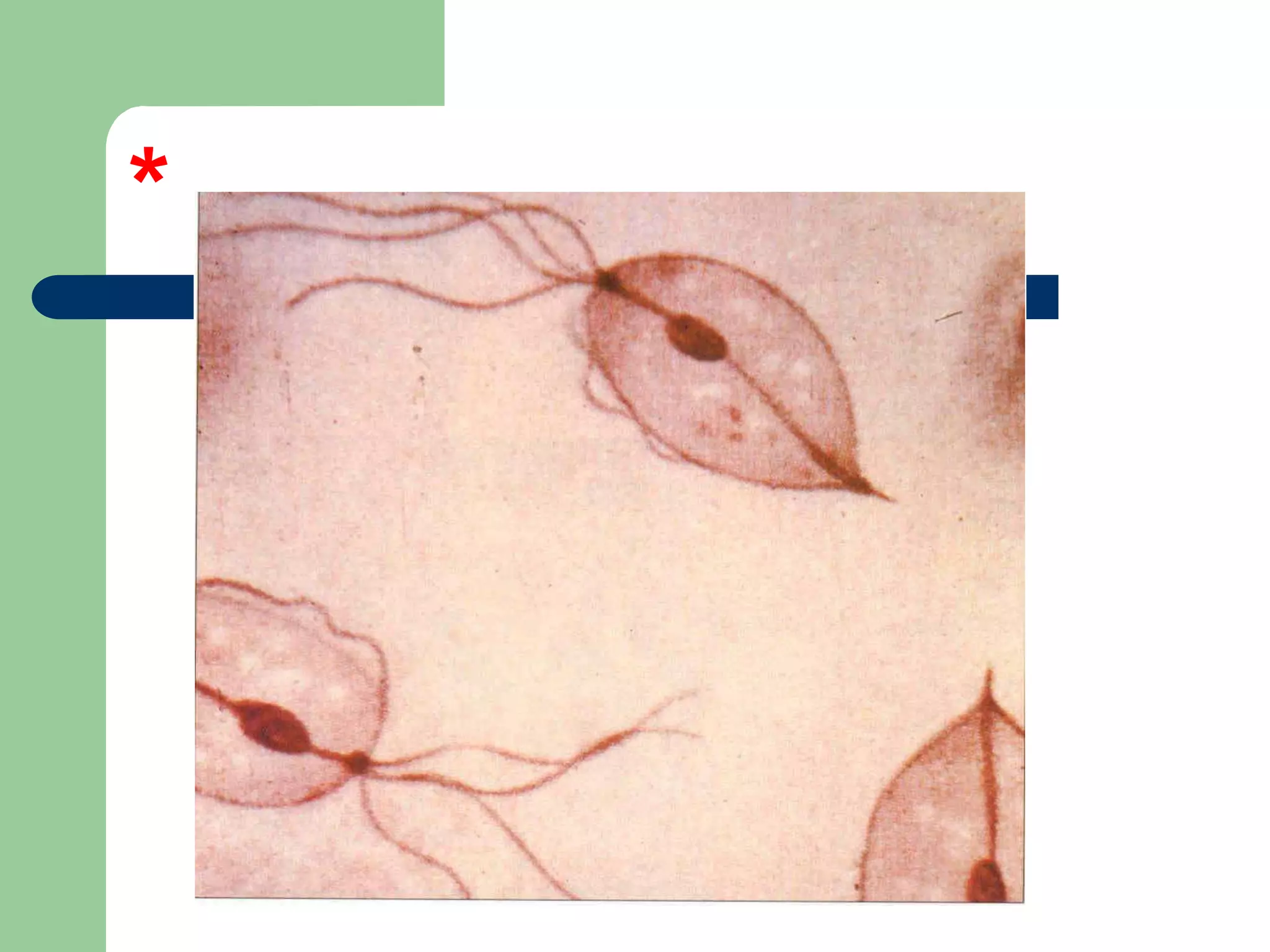
Qs:
1. Name thisorganism.
2. How would it present clinically?
3. What is the treatment?
4. Would you treat the partner? Why?
23.
1. Trichomonus vaginalis.
2.It could present with itching and discharge.
3. Treat with metronidazole.
4. Yes treat the husband, because it is
infectious sexually transmitted disease.
Qs:
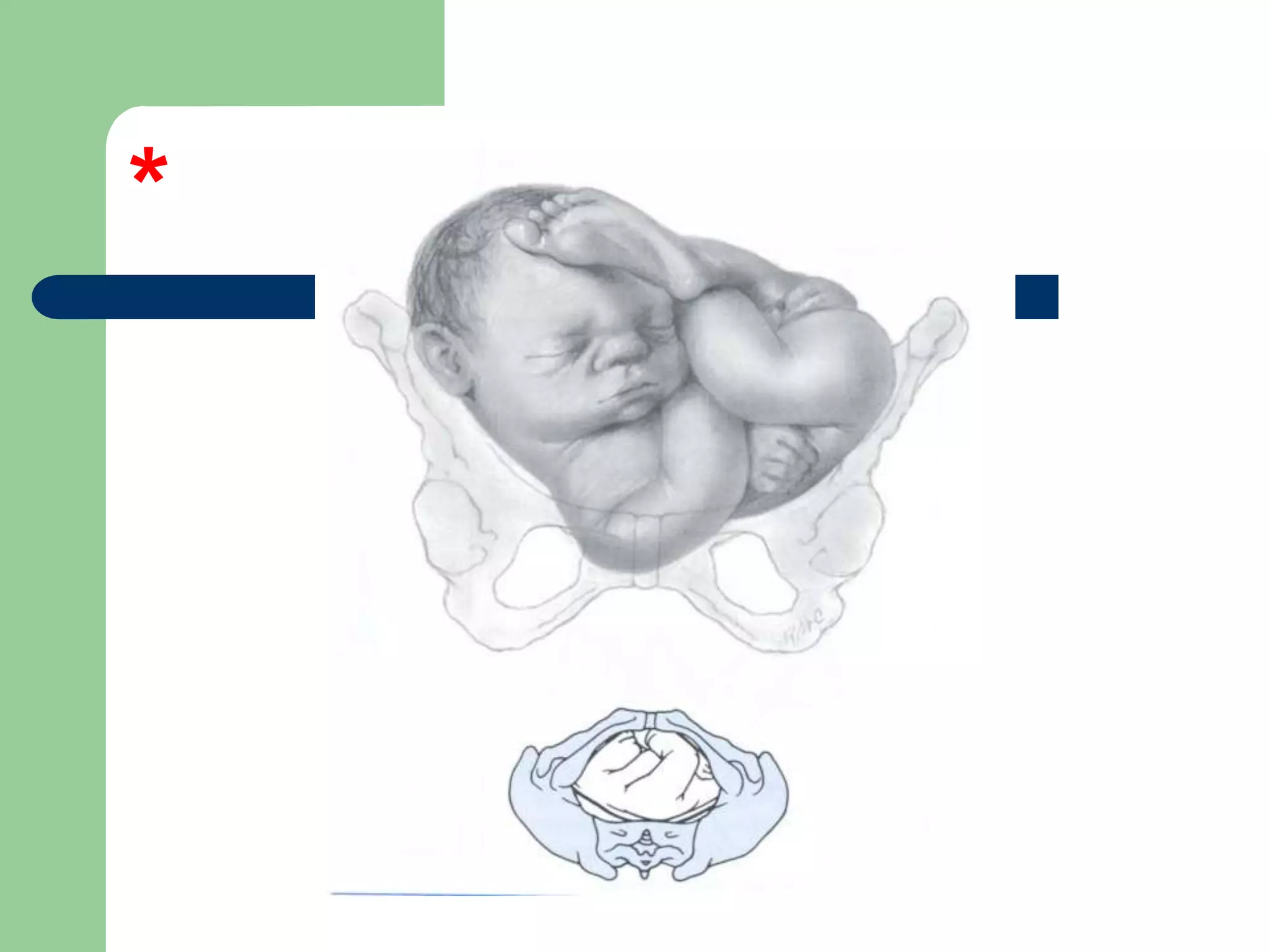
1. What isthe lie and presentation?
2. Name two diagnostic signs.
3. Name two complications.
4. What is the management:
Before delivery?
During labour?
46.
1.Transverse lie, shoulderpresentation.
2.Signs: low fundal hight to date, feel the head on
abdominal lateral sides, feel the back of the fetus
running transverse lie, transverse lie by US.
3.Complications: cord prolapse (Most common), cord
compression, shoulder dystocia, prolonged labour,
fetal distress, maternal exhaustion, fetal injury, bone
fracture, maternal injury and obstructed labour.
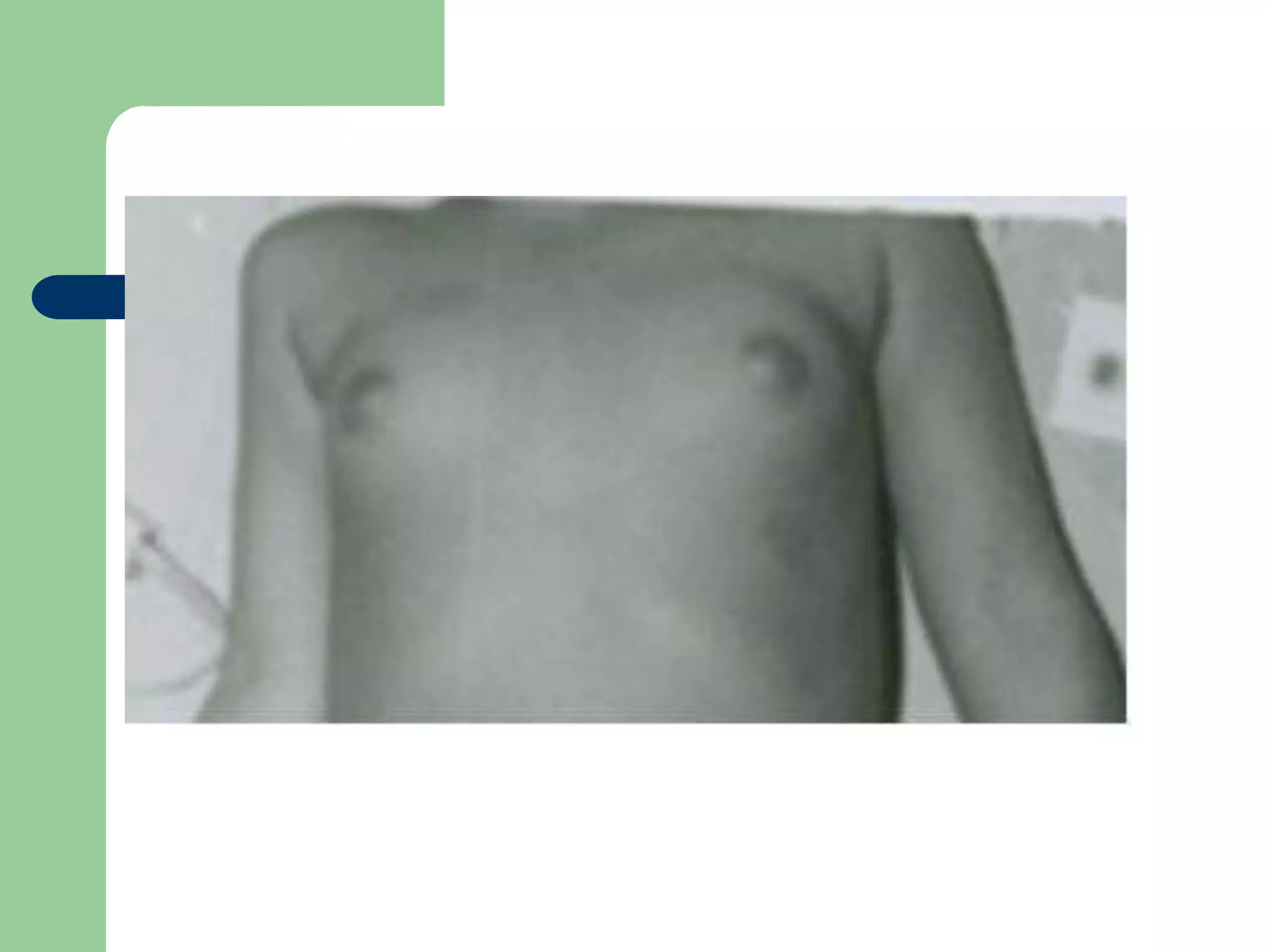
Qs
1. What doyou see?
2. Give two DD
3. What would you ask in H. (give 3)
4. What would you order for investigation.
(give 3)
50.
What doyou see?
Breast budding.
Give 2 DD.
1. Complete precocious puberty.
2. Incomplete precocious puberty
51.
What wouldyou ask in H?
1. Ask if she has any pubic or axillary hair?
2. Ask if she had any vaginal bleeding or
menses.
3. Ask if she has been taking any medications
4. Ask for any family H in this condition.
52.
What wouldyou order for investigation?
1. Check hormonal level of estrogen.
2. Check her FSH, LH levels.
3. Take radio-images of her brain to rule out
any secretery tumors (sp: pituitary)
4. Do an US for her ovaries to rule out any
estrogen secreting tumors (ex: granulosal
cells tumor)
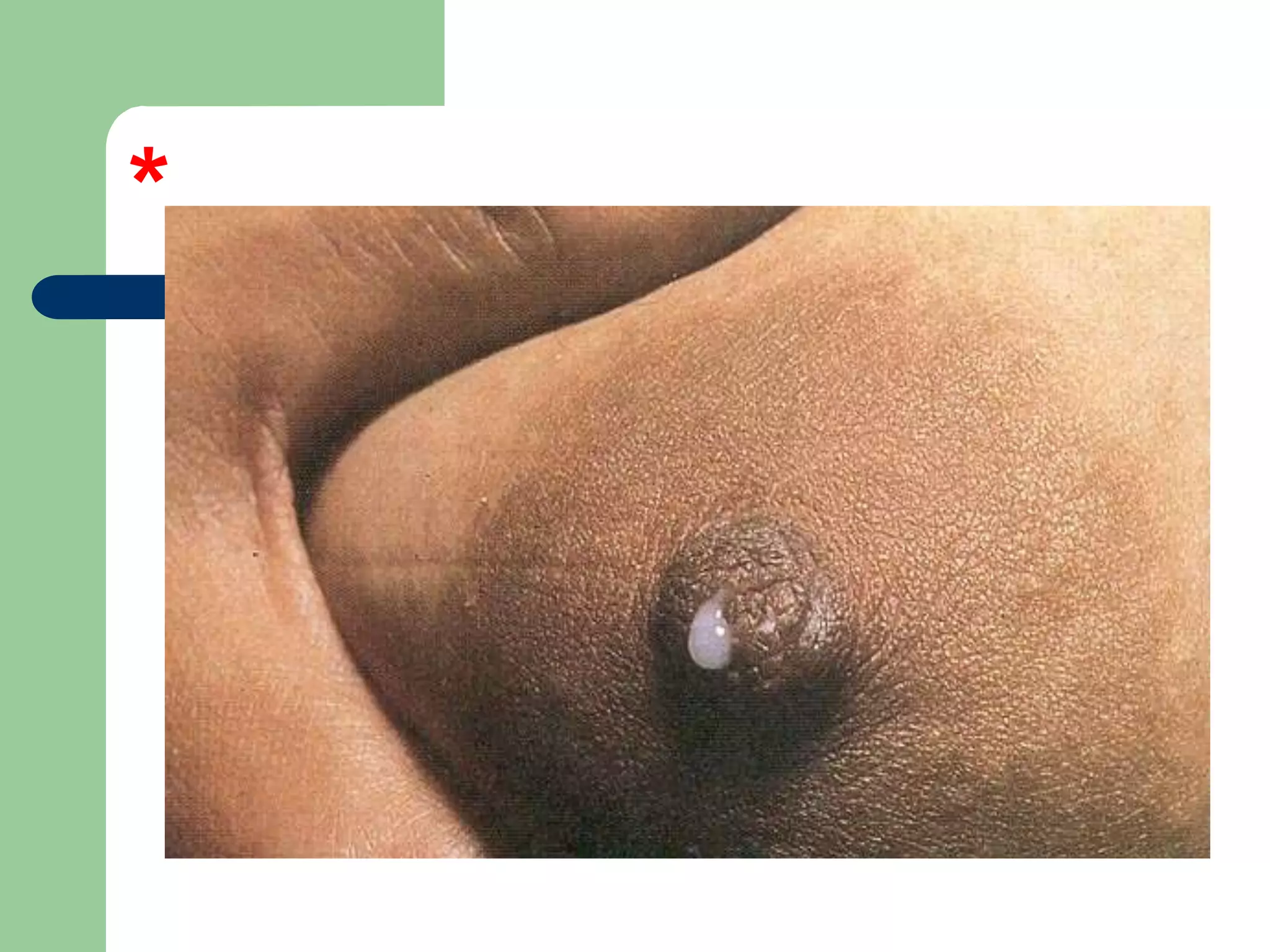
Qs
1. What isthis condition?
2. Caused by which hormone?
3. What could cause it elevation?
4. What other posible symptoms could it
present with?
5. How would you treat it?
55.
What isit?
Galactorrhea
By which hormone?
Prolactin
56.
What couldcause its elevation? (give 4)
Physiological (lactating breast-feeding
mother)
Pituitary adenoma
Drug-induced.
Other prolactin-secretory tumors.
Idiopathic elevation.
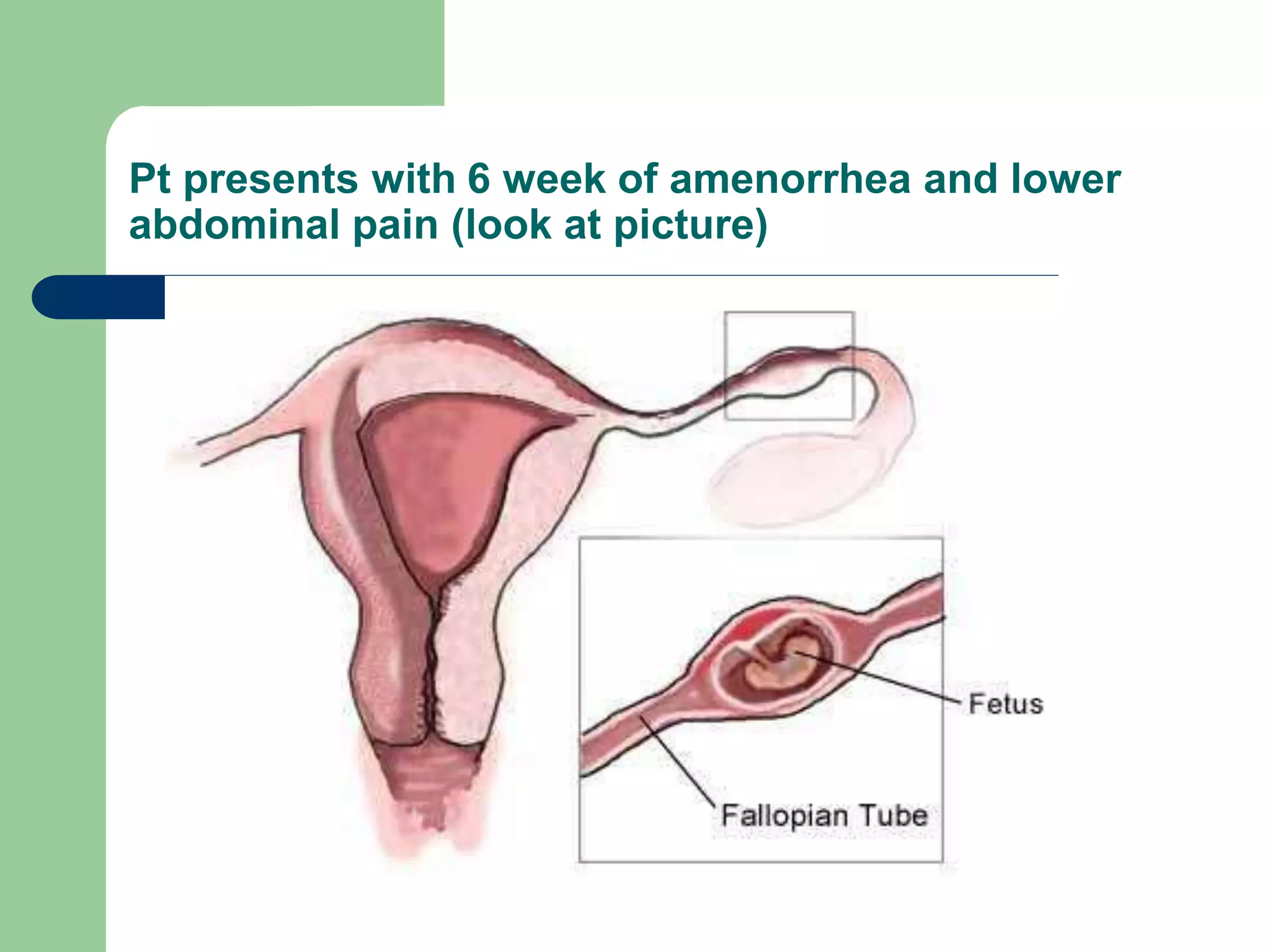
Pt presents with6 week of amenorrhea and lower
abdominal pain (look at picture)
61.
Qs
What isthe DD?
What possible other symptoms?
Give 4 risk factors.
How would you treat?
62.
What isthe Dd?
Ectopic pregnancy.
What possible other symptoms?
PV bleeding, lower abdominal pain and
amenorrhea
63.
Give 4risk factors.
Previous Ectopic pregnancy
Tubal disease
Chronic PID and adhesions.
Adhesions from endometriosis
IUCD
Tubal ligation
64.
How wouldyou manage?
Medical: methotrexate if it fits the
recommended criteria.
Surgical: salpingostomy (if in ampulla and
uncomplicated) salpingectomy if otherwise
with checking the patency and health of the
other tube.
Qs
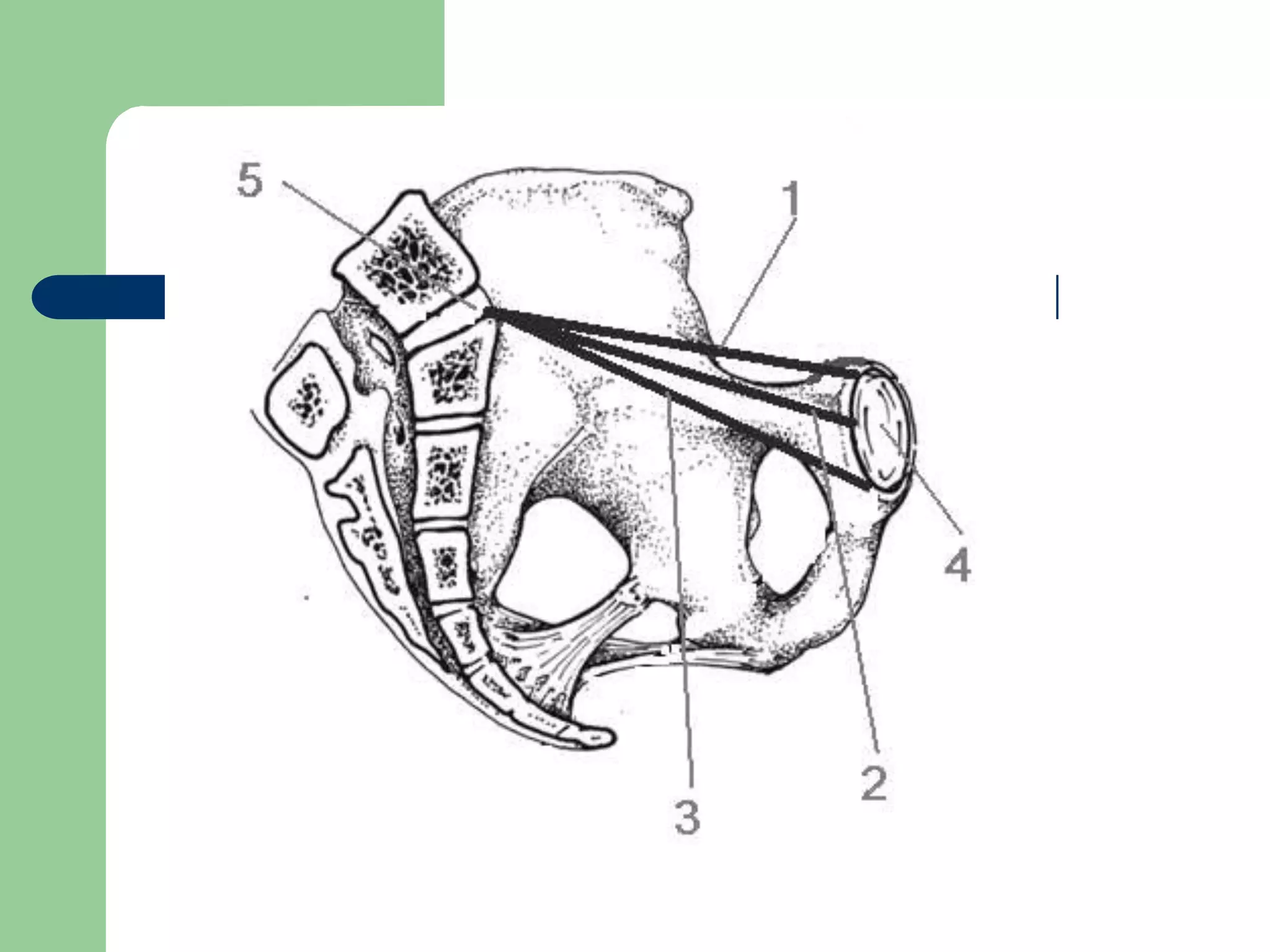
1. What are1, 2 ,3 ?
2. Which one is the most important
obstetrically and what’s its length?
3. What are 4 and 5?
68.
What are1, 2 and 3?
1= True (anatomic) diameter.
2=obstetric diameter.
3=diagonal diameter.
Which is obs. Imp and what’s its length?
Obstetric diameter and its about 11.5 cm
69.
1. What are4 and 5?
4=pubic bone (symphesis pubis)
5=sacral promontory.
Qs
1. What isyour DD?
2. What symptoms would present (give 2)
3. What hormones would be elevated?
4. How would you treat?
73.
What isthe DD?
Polycystic ovarian syndrome (PCOs)
Symptoms:
Acne
Hiristisum
Infertility
Irregular menses
74.
What hormoneswould be elevated?
(Give2)
1. LH
2. Androgens
3. Insulin
75.
How wouldyou treat?
Give combined OCPs (for hiristisum and
prevention of endometrial cancer due to
elevated unopposed estrogen
Or give progestrone to prevent endometrial
cancer
Give metformin for insulin resistance.
Remove ovary surgically if associated with
neoplasm or unreasoning to medications.
Qs
What are1 and 2?
Name 4 indications for C/S.
Name 4 complications for C/S.
91.
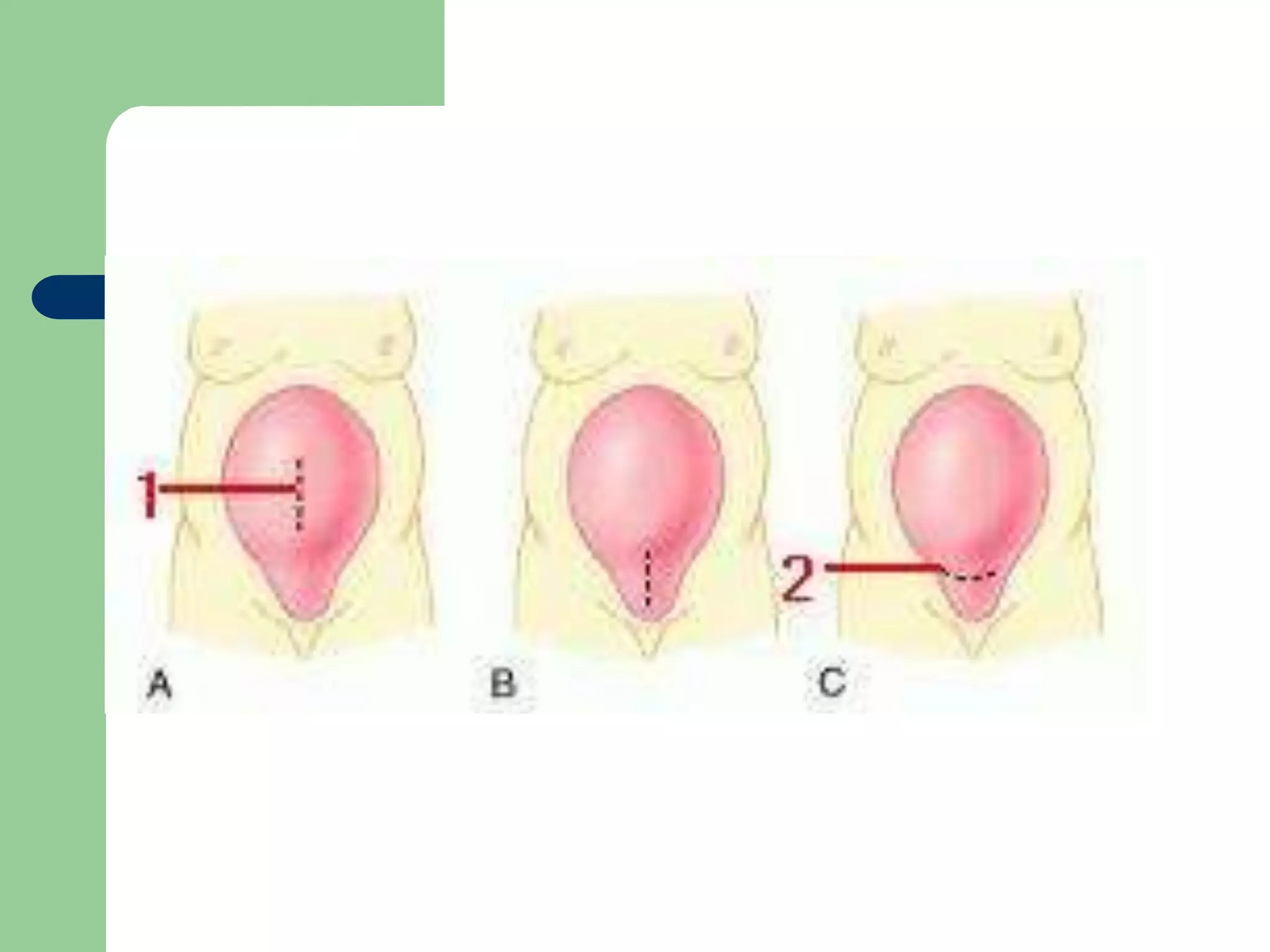
What are1 and 2?
1= vertical (longtudinal) section (classic)
2= low transverse section.
92.
Name 4indications.
1. Placenta prevea.
2. Preveious myomectomy
3. Previous C/S
4. Previous uterine rupture
5. Conditions need to deliver baby as fast as possible
with the cervix is unfavourable like:
A-Severe pre-eclampsia
B-Eclampsia.
C-Severe fetal distress.
93.
Name 4complications:
Heavy bleeding.
risk of uterine rupture in a subsequent pregnancy.
Higher risk for infections and puerperal sepses.
Urine overflow incontinence (from anaesthetics)
Risk of fetal injury (from cutting the uterus)
Injury of other pelvic organ tissues.